SMS 2011 December;17(2):86-94.
Published online 2011 December 30 |
| Copyright ⓒ 2010 Soonchunhyang Medical Science
|
| Clinical Usefulness of 64-Channel Multidetector Computed Tomography, Capsule Endoscopy, and Double-Balloon Enteroscopy in Obscure Gastrointestinal Bleedings |
| Jun Seok Park, Jin Oh Kim, Hyun Gun Kim, Joon Seong Lee, Tae Hee Lee, Seong Ran Jeon, Byung Kyu Ahn, Min Jeong Kim, Jin Young Yoo |
| Department of Internal Medicine, Soonchunhyang University Seoul Hospital, Seoul, Korea |
| Corresponding Author: Jin Oh Kim , Tel: +82-2-709-9345 , Fax: +82-2-795-3687 , Email: jokim@schmc.ac.kr
|

|
ABSTRACT
|

|
|
|
Objective: Obscure gastrointestinal bleeding primarily originates from small-bowel lesions. It is difficult to detect the lesions by using classical diagnostic modalities, and thus, new methods have been developed. The aim of study was to evaluate the clinical usefulness of 64-channel multidetector computed tomography, capsule endoscopy, and double-balloon enteroscopy for detection of obscure gastrointestinal bleeding. Methods: This retrospective study analyzed the findings of 64-channel multidetector computed tomography, capsule endoscopy, and double-balloon enteroscopy in patients with obscure gastrointestinal bleeding treated at Soonchunhyang University Seoul Hospital between January 1, 2008 and September 30, 2010. Results: Five of 22 positive findings (22.7%) were obtained using 64-channel multidetector computed tomography. The computed tomography could not detect active bleeding lesions but it played an important role on the evaluation of extraluminal lesions. The diagnostic yield of capsule endoscopy was 82.4%. No cases of capsule retention were detected in this study. Bleeding lesions were identified in all cases through the use of double-balloon enteroscopy. One hemoclipping and 2 biopsies were performed. Conclusion: Sixty-four-channel multidetector computed tomography can be used to evaluate extraluminal lesions. Capsule endoscopy is the most convenient endoscopy method. Invasive procedures can be performed using double-balloon enteroscopy. These methods can be used complementarily to diagnose and treat occult gastrointestinal bleeding. Use of capsule endoscopy after screening with 64-channel multidetector computed tomography in the case of patients with occult gastrointestinal bleeding is suggested. In case of lesions wherein invasive procedures are required, use of double-balloon is preferred. |
|
Keywords: Obscure gastrointestinal bleeding; Multidetector computed tomography; Capsule endoscopy; Double-balloon enteroscopy |
|
|
|
서론
|
|
|
원인 불명의 위장관 출혈은 상부위장관내시경, 대장내시경이나 고식적인 영상의학검사로 원인을 찾지 못하는 위장관 출혈이 계속되거나 반복되는 경우를 말한다. 이는 전체 위장관 출혈의 5% 정도로 추정되며, 대부분은 소장에서 발생한다
[1]
. 소장은 해부학적인 위치와 특성 때문에 일반적인 내시경으로는 그 전체를 관찰하기 어렵다. 이같은 문제를 해결하기 위해서 내시경 분야에서는 캡슐내시경, 이중풍선소장내시경 등 새로운 진단 도구가 개발되어 사용 중이다
[2,3]
. 영상의학 분야에서도 컴퓨터단층촬영의 경우, 다중검출 기술이 개선되고 조영 기술 등이 발전하여 소장을 자세하게 관찰할 수 있게 되었다.
새로 개발된 검사 방법들은 보급률이 낮고, 비용적인 부담도 크다
[4]
. 또 검사자와 장비에 따른 결과 편차가 크고, 표준 검사 방법이 확립되어 있지 않다
[5]
. 빠른 진단과 치료가 필요한 원인 불명의 위장관 출혈 환자에 어떤 검사를 시행해야 할지는 각 검사의 장단점 및 비용 등을 신중하게 고려하여 결정해야 한다. 이에 본 연구에서는 원인 불명의 위장관 출혈 환자를 대상으로 64채널 다중검출 컴퓨터단층촬영과 캡슐내시경 또는 이중풍선소장내시경을 시행한 결과를 분석함으로써 그 임상적 유용성을 알아보고자 하였다. |
|
|
대상 및 방법
|
|
|
1. 대상
2008년 1월 1일부터 2010년 9월 30일까지 순천향대학교 서울병원에서 원인 불명의 위장관 출혈에 대해 치료를 받은 환자는 56명이었다. 이들 중 생체징후가 안정적이고 이전 검사기록이 없는 22명을 대상으로 64채널 다중검출 컴퓨터단층촬영과 캡슐내시경 또는 이중풍선소장내시경을 시행한 결과를 후향적으로 분석하였다
(Fig.1)
.
2. 방법
1) 64채널 다중검출 컴퓨터단층촬영
검사 대상에 포함된 22명의 환자 모두에게 64채널 다중검출 컴퓨터단층촬영을 시행하였다. 8시간 이상 금식 후에 SOMATOM Sensation 64 (Siemens AG, Medical Solutions, Forchheim, Germany)를 사용하여 촬영하였다. 22명 중 7명은 경구 중성 장관조영제(oral neutral enteral contrast) 없이 조영 전기 영상을 얻고, iodine (320-350 mg/mL) 조영제 140 mL를 3 mL/sec 속도로 정맥 내 투여한 후 각각 30초, 70초 만에 동맥기, 지연기 영상을 얻었다. 15명은 경구 중성 장관조영제로서 4.4% sorbitol 용액 1,800 mL를 40분에 걸쳐 분복하고 조영 전기 영상을 얻었고, iodine (320-350 mg/mL) 조영제 140 mL를 3 mL/sec 속도로 정맥 내 투여한 다음, 45초 만에 동맥기 영상을 얻고 70초 만에 지연기 영상을 얻었다.
2) 캡슐내시경
64채널 다중검출 컴퓨터단층촬영에서 궤양이나 종괴가 발견된 3명의 환자를 제외하고 19명의 환자에게 캡슐내시경을 시행하였다. 모두 12시간 이상 금식 후에 검사를 시행하였고, 이전 검사 결과를 바탕으로 장관 전처치가 필요한 7명은 polyethylene glycol (Colyte)을 복용하였다. 검사 장비로는 11×24 mm 크기를 갖고 초당 3장의 영상을 얻을 수 있는 MicroCam (Intromedic, Seoul, Korea)과 11×26 mm 크기를 갖고 초당 2장의 영상을 얻을 수 있는 SB2 (Given imaging, Yoqneam, Israel)를 사용하였다. 환자가 캡슐을 삼키고 1시간 뒤에 단순복부촬영으로 캡슐의 소장 진입 여부를 확인하였고, 금식을 유지한 상태에서 검사를 진행하였다. 각 캡슐내시경의 배터리 가용시간을 고려하여 감지기와 기록기를 제거하고, MicroCam으로 얻은 정보는 MiroView (Intromedic)로 얻은 정보는 Rapid Software Suite (Given imaging, Yoqneam, Israel)를 사용하여 식별 가능한 영상으로 변환하여 판독하였다.
3) 이중풍선소장내시경
64채널 다중검출 컴퓨터단층촬영에서 궤양이나 종괴가 발견된 3명과 캡슐내시경에서 조직검사나 치료 시술 등이 필요한 병변이 발견된 3명을 포함하여 총 6명의 환자를 대상으로, 한 사람의 숙련된 시술자가 방사선 투시하에 이중풍선소장내시경 EN-450P5/20, T5/20 (Fujinon Inc., Saitama, Japan)을 사용하여 검사하였다.
경구 삽입 시에는 12시간 이상 금식 후에, 경항문 삽입 시에는 polyethylene glycol (Colyte)을 이용한 장 정결 후에 검사를 시행하였다. 내시경 진입 방향은 환자의 임상 병력과 이전 검사 소견을 참고하여 결정하였으며, 처음 진입한 방향에서 병변을 발견하지 못했을 때에는 내시경의 최대 도달 지점의 점막 표면에 India ink로 표시한 후, 반대쪽 접근을 시도하였다.
모든 검사는 midazolam을 이용한 의식하 진정상태에서 시행되었으며, 검사 시행 전 pethidine hydrochloride 50 mg을 근육 내 주사하고, 검사 도중 환자가 각성하거나 통증을 심하게 호소하면 midazolam과 pethidine hydrochloride를 추가 투여하였다. 명확한 출혈 병변이 발견되거나 내시경의 진입이 어려워진 경우에는 검사를 중단하였다. |
|
|
결과
|
|
|
연구 대상에 포함된 22명의 환자 중 남자는 15명, 여자가 7명이었으며, 대상자의 나이는 22세부터 78세로 그 중앙값은 58세였다. 20명의 환자에서 흑색변, 혈변 등 위장관 출혈 증상이 발생한 지 14일 이내에 소장에 대한 검사를 시행하였다. 2명은 철 결핍성 빈혈에 대한 원인 규명 과정에서 반복되는 위장관 출혈 증상을 호소하였거나, 대변 잠혈 반응 양성 소견을 보여 검사하였다.
1. 64채널 다중검출 컴퓨터단층촬영
원인 불명의 위장관 출혈에서 경구 중성 장관조영제 복용 여부와 상관없이 64채널 다중검출 컴퓨터단층촬영의 소장 병변 진단율은 22.7%였다. 경구 중성 장관조영제 복용 후에 시행한 15예 중 3예(20%)에서, 경구 중성 장관조영제를 복용하지 않고 시행한 7예 중 2예(28.5%)에서 소장 병변을 발견하였다
(Table 1)
. 이들의 추정 진단은 메켈게실 출혈 1예, 소장 정맥류 1예, 종주 궤양이 동반된 만성 염증성 장 질환 1예, 소장의 위장관 기질 종양 2예였다.
장관 외부로 돌출되는 소장 종괴 1예에서 이중풍선소장내시경을 시행하였으나 근위부 공장의 궤양 출혈만이 관찰되었다. 64채널 다중검출 컴퓨터단층촬영 소견을 바탕으로 근치적 치료를 결정하고 부분 소장절제술을 시행하였다. 이를 통해 근위부 공장의 종괴와 내강에서 관찰된 궤양은 동일 병변임을 확인하고
(Fig.2)
면역조직화학염색에서 CD117 양성인 위장관 기질 종양으로 확진하였다.
2. 캡슐내시경
22명의 환자 중에서 19명에게 캡슐내시경을 시행하였다
(Fig.1)
. 장관 전처치를 받은 환자는 8명이었고, 11명은 금식만 유지한 채 검사를 시행하였다. MicroCam을 사용한 경우가 10예, SB2를 사용한 경우가 9예였다
(Table 2)
. 검사 시간 동안 캡슐이 회맹판에 도달하지 못하여 전체 소장을 관찰할 수 없던 경우가 1예(5.2%) 있었으나, 공장의 궤양을 진단할 수는 있었다. 캡슐내시경에서 출혈 가능한 병변을 발견한 경우는 16예(84.2%)로 미란 및 궤양 11예, 혈관형성 이상 4예, 소장 정맥류 1예 순이었다. 소장 용종 2예를 포함하여 총 3예(15.8%)에서 출혈성 병변을 발견할 수 없었다
(Table 2)
. 64채널 다중검출 컴퓨터단층촬영과 이중풍선소장내시경에서 확인된 공장의 게실 출혈을 발견하지 못한 경우가 1예 있었으며, 장관 내 캡슐 정체는 발생하지 않았다.
소장 정맥류 1예에서 64채널 다중검출 컴퓨터단층촬영으로는 실제 출혈 여부를 확인하기 어려웠으나, 캡슐내시경으로 출혈을 확인하고 색전술을 시행하여 치료하였다
(Fig.3)
.
3. 이중풍선소장내시경
6예의 이중풍선소장내시경 중에서 검사 도중 십이지장 궤양 출혈을 발견한 1예와 캡슐내시경으로 진단한 공장 궤양을 조직검사하기 위해 시행한 1예는 경구 접근만 하였고, 나머지 4예는 경구 및 경항문 접근 모두를 시행하였다. 6예(100%)에서 출혈 병변을 발견하였고, 궤양 4예, 게실 출혈 1예, 소장 종괴 1예 순이었다
(Table 3)
.
64채널 다중검출 컴퓨터단층촬영 결과, 만성 염증성 장 질환이 의심된 1예에서 이중풍선소장내시경을 시행하였다. 근위부 공장의 궤양 출혈을 클립 지혈술로 치료하고, 공장 중반부의 궤양에서 조직검사를 시행하여 크론병을 확진하였다
(Fig.4)
. |
|
|
고찰
|
|
|
원인 불명의 위장관 출혈은 약 75%에서 소장에 원인이 있는 것으로 보고되고 있는데 일반적인 내시경검사로는 소장에의 접근이 어려워 다양한 검사 방법이 개발되고 있다
[6]
. 컴퓨터단층촬영은 다중검출 기술 및 컴퓨터 기술이 발전하면서 검사의 정확성이 높아지고 있다. 조영제 사용에 따른 부담이 있고 내시경보다 점막 병변에 대한 진단율이 떨어지는 단점이 있으나 64채널 다중검출 기술, 3차원 재구성 기술, 기타 조영 기술 및 고위관장술을 응용하면, 그 정확성을 높일 수 있다
[7-10]
. 이에 원인 불명의 위장관 출혈에서 그 진단율이 45%까지 보고되고 있다
[9]
. 또한 장관동맥루, 혈담, 출혈이 동반된 췌장염 등 장관 외부에 출혈 원인이 있는 경우, 컴퓨터단층촬영이 도움이 될 수 있다.
본 연구에서는 원인 불명의 위장관 출혈 환자에서 64채널 다중검출 컴퓨터단층촬영의 소장 병변 진단율은 22.7%였는데, 이는 앞서 언급된 45%보다 떨어지는 결과이다
(Table 4)
. 고위관장술까지 시행된 경우가 없었고 경구 중성 장관조영제 복용 여부에 따라 검사 방법이 양분되었으며, 두 경우에서 정맥 내 조영제 투여 후 영상을 얻는 시간에 차이가 있었던 것이 원인으로 여겨진다.
원인 불명의 위장관 출혈에서 캡슐내시경의 진단율은 38-83% 정도로 보고되고 있다
[11]
. 환자가 캡슐을 삼키면 장관의 연동 운동에 의해서 기기가 이동하므로 자극이 적다는 장점이 있으나 병변을 능동적으로 관찰할 수 없는 것이 단점이다. 또 배터리의 한계 때문에 검사 시간에 제한이 있어 전체 소장을 검사하지 못할 수도 있다. 캡슐 정체 등의 부작용 때문에 삼킴 곤란이나 장폐색, 협착 등이 있으면 검사할 수 없고 크론병이나 결핵성 장염 등의 만성 염증성 장 질환, 위장관 종괴가 의심되는 경우에도 주의해야 한다
[4]
.
본 연구에서는 검사 시간 내에 캡슐이 회맹판까지 도달하지 못하여 전체 소장을 관찰할 수 없었던 경우가 1예 있었다. 캡슐 정체는 발생하지 않았는데 64채널 다중검출 컴퓨터단층촬영 결과를 바탕으로 장관 협착, 종괴 등 캡슐 정체를 일으킬 만한 병변이 있던 3명의 환자에서 캡슐내시경을 시행하지 않은 것이 도움이 되었을 것으로 생각한다.
이중풍선소장내시경의 소장 질환에 대한 진단율은 60-80% 정도로 보고되고 있다[12-14]. 병변을 능동적으로 관찰할 수 있고 조직 생검, 용종 절제, 지혈, 협착부위 확장 등 침습적인 시술이 가능하다는 장점이 있으나 국내 보급률이 낮고, 비용이 비싸므로 널리 이용되고 있지 않다[3,13,15]. 또 검사를 받는 환자가 느끼는 불편감이 크고, 검사 시간도 길어서 시술자의 노력이 많이 들고, 그 숙련도에 따른 결과 차이가 크다
[15,16]
.
각 검사의 소장 병변에 대한 진단 능력을 분석하는 시도도 많이 이루어지고 있다. 적은 모집단 수로 인해 다소 견해 차이를 보이고 있으나, 아직 어느 검사도 절대적인 우월성을 입증하지는 못하고 있다. 원인 불명의 위장관 출혈에서 캡슐내시경과 이중풍선소장내시경의 진단율을 연구한 11개 자료를 메타 분석한 결과, 각각 65% 대 57% (IYw: 3%)로 비슷하였다
[5]
. 또 소장 병변에 대하여 캡슐내시경과 이중풍선소장내시경의 진단 일치도를 연구한 자료에서도 두 검사는 kappa=0.48 (95% confidence interval, 0.44-0.52, P<0.05)로 중등도의 일치도를 보인 바 있다
[4]
.
다중검출 컴퓨터 단층촬영에서 고위관장술을 시행하면 점막 병대한 민감도를 높일 수 있다
[9]
. 원인 불명의 위장관 출혈에서 고위관장술을 시행한 다중검출 컴퓨터단층촬영과 캡슐내시경을 비교한 자료를 살펴보면, 민감도가 69% (41-89%) 대 87% (62-98%), 특이도가 100% (79-100%) 대 81% (54-96%), 95% 신뢰 구간 내에서의 정확도가 84% (67-95%) 대 84% (67-95%)로 유사한 성적을 보이고 있다
[17]
.
본 연구는 원인 불명의 위장관 출혈을 진단하고 치료하는 과정에서 64채널 다중검출 컴퓨터단층촬영과 캡슐내시경, 이중풍선소장내시경의 임상적 유용성을 실제 증례 분석을 통하여 제시하였다는 것에 그 의의를 둘 수 있으나, 모집단 수가 적어서 통계적인 의미가 부족하다.
원인 불명의 위장관 출혈이나 소장 질환 환자에서 다중검출 컴퓨터단층촬영, 캡슐내시경, 이중풍선소장내시경의 진단율, 진단 일치도, 임상적 효용성 등을 알아보기 위하여 시행된 대규모 전향적 연구는 아직 없다. 이는 캡슐내시경, 이중풍선소장내시경의 검사 비용이 고가이고 그 보급률이 낮아서 제한된 연구 기관에서의 적응이 불가피하기 때문이다
[4]
.
원인 불명의 위장관 출혈은 증상 재발이 빈번하므로 방사선 피폭량을 고려하면 매 출혈 시마다 컴퓨터단층촬영을 시행할 수는 없다. 기존의 연구들을 살펴보면 컴퓨터단층촬영을 시행하는 적응증이 정확히 정립되어 있지 않다. 또 경구 중성 장관조영제로 사용된 약품이나 복용 방법 등에 차이가 있다[7,9,18,19].
64채널 다중검출 컴퓨터단층촬영, 캡슐내시경, 이중풍선소장내시경 등 새로 개발된 검사 방법들은 원인 불명의 위장관 출혈 환자에서 소장을 검사하는 데에 많은 발전을 가져온 것이 사실이다. 하지만 진단, 치료에 있어 표준으로 적용되기엔 임상적 경험이 아직 부족하다.
본 연구에서 살펴본 바를 정리하면 원인 불명의 위장관 출혈 환자에서 64채널 다중검출 컴퓨터단층촬영은 출혈 병소를 직접 확인하기에는 적합하지 않으나, 내시경검사에 부적응이 되는 병변을 사전에 확인할 수 있고, 장관 외부의 병변이나 주변 혈관의 상태를 평가할 수 있다. 이후 소장검사에는 캡슐내시경을 우선 고려하되 캡슐 정체를 일으킬 만한 병변이나 조직검사, 치료 시술 등이 필요한 병변이 발견된 경우에는 이중풍선소장내시경을 시행하는 것으로 검사 시행에 따른 환자의 부담을 최소화할 수 있다. 하지만 이를 임상에 적용하기 위해서는 대규모 연구를 통해 검사의 적응증을 확립하고 방법을 표준화하는 작업이 선행되어야 한다. |
|
|
|
FIGURES
|
|
|

|
Fig.1
The enrollment algorism of the study. OGIB, obscure gastrointestinal bleeding; MDCT, multidetector computed tomography; CE, capsule endoscopy; DBE, double-balloon enteroscopy; IBD, inflammatory bowel disease. |

|
|
Fig.2
A case of exophytic gastrointestinal stromal tumor. (A, B) Computed tomography scans show a central low-attenuated mass, protruding out from the small intestine in the pelvic cavity (arrows); this mass was highly suspected to be a gastrointestinal stromal tumor (GIST). (C) Through double-balloon enteroscopy, a hemorrhagic ulcer was found in the jejunum (arrow). The suspected GIST was surgically removed and diagnosed as a CD117-positive mass containing central necrosis with hemorrhage. The mass has an ulcer on its luminal side. |
|
|

|
Fig.3
A case of jejunal variceal bleeding. (A) With three-dimensional reconstruction technology, a computed tomography scan shows tortious and dilated multiple collateral vessels (arrow) originating from the left iliac vein and draining into the jejunal branch of the superior mesenteric vein. (B) Attenuation of the associated distal jejunum is high (arrow). (C) The visual field of the capsule endoscopy is poor because of active bleeding in the jejunum. (D) Two embolization coils were applied to the proximal portion of the varix (arrow). |
|
|

|
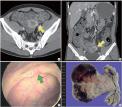
Fig.4
A case of Crohn’s disease. (A, B) Multifocal areas of longitudinal ulcers in the pelvic and distal ileal loops with wall thickening (arrows). (C) In an oral approach of double¬-balloon enteroscopy, a hemoclip is applied to the jejunal ulcer bleeding. (D) In an anal approach of double-balloon enteroscopy, many ulcerative lesions can be seen (arrow). Biopsies were performed on the ulcerative lesions, and Crohn’s disease was diagnosed on the basis of pathologic findings. |
|
|
|
|
|
TABLES
|
|
|

|
Table.1
Findings of the 64-channel MDCT in the patients with obscure gastrointestinal bleeding |
|
|

|
Table.2
Findings of the capsule endoscopy in the patients with obscure gastrointestinal bleeding |
|
|

|
Table.3
Findings of double-balloon enteroscopy in the patients with obscure gastrointestinal bleeding |
|
|

|
Table.4
Comparison of findings between the patients with obscure gastrointestinal bleeding |
|
|
|
| |
|
|
REFERENCE
|
|
|
|
1.
|
Lewis BS. Small intestinal bleeding. Gastroenterol Clin North Am 1994; 23:67-91. |
|
2.
|
Iddan G, Meron G, Glukhovsky A, Swain P. Wireless capsule endoscopy. Nature 2000;405:417. |
|
3.
|
Yamamoto H. Double-balloon endoscopy. Clin Gastroenterol Hepatol 2005;3(7 Suppl 1):S27-9. |
|
4.
|
Kim HG, Kim JO, Lee TH, Kim WJ, Chol HS, Cho YK, et al. Diagnostic agreement between capsule endoscopy and double-balloon enteroscopy of small bowel disease. Korean J Gastrointest Endosc 2010;40:236-43. |
|
5.
|
Pasha SF, Leighton JA, Das A, Harrison ME, Decker GA, Fleischer DE, et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin Gastroenterol Hepatol 2008;6:671-6. |
|
6.
|
Pennazio M, Arrigoni A, Risio M, Spandre M, Rossini FP. Clinical evaluation of push-type enteroscopy. Endoscopy 1995;27:164-70. |
|
7.
|
Horton KM, Fishman EK. The current status of multidetector row CT and three-dimensional imaging of the small bowel. Radiol Clin North Am 2003;41:199-212. |
|
8.
|
Patak MA, Mortele KJ, Ros PR. Multidetector row CT of the small bowel. Radiol Clin North Am 2005;43:1063-77, viii. |
|
9.
|
Huprich JE, Fletcher JG, Alexander JA, Fidler JL, Burton SS, McCullough CH. Obscure gastrointestinal bleeding: evaluation with 64-section multiphase CT enterography--initial experience. Radiology 2008;246:562-71. |
|
10.
|
Jang HJ, Park CH, Han SY, Byun HW, Choi MH, Kae SH, et al. Comparison of double balloon enteroscopy and capsule endoscopy for patients with suspected small bowel diseases. Korean J Gastrointest Endosc 2007; 35:379-84. |
|
11.
|
Rondonotti E, Villa F, Mulder CJ, Jacobs MA, de Franchis R. Small bowel capsule endoscopy in 2007: indications, risks and limitations. World J Gastroenterol 2007;13:6140-9. |
|
12.
|
Yamamoto H, Kita H, Sunada K, Hayashi Y, Sato H, Yano T, et al. Clinical outcomes of double-balloon endoscopy for the diagnosis and treatment of small-intestinal diseases. Clin Gastroenterol Hepatol 2004;2:1010-6. |
|
13.
|
May A, Nachbar L, Ell C. Double-balloon enteroscopy (push-and-pull enteroscopy) of the small bowel: feasibility and diagnostic and therapeutic yield in patients with suspected small bowel disease. Gastrointest Endosc 2005;62:62-70. |
|
14.
|
Nakamura M, Niwa Y, Ohmiya N, Miyahara R, Ohashi A, Itoh A, et al. Preliminary comparison of capsule endoscopy and double-balloon enteroscopy in patients with suspected small-bowel bleeding. Endoscopy 2006;38:59-66. |
|
15.
|
Heine GD, Hadithi M, Groenen MJ, Kuipers EJ, Jacobs MA, Mulder CJ. Double-balloon enteroscopy: indications, diagnostic yield, and complications in a series of 275 patients with suspected small-bowel disease. Endoscopy 2006;38:42-8. |
|
16.
|
Zhong J, Ma T, Zhang C, Sun B, Chen S, Cao Y, et al. A retrospective study of the application on double-balloon enteroscopy in 378 patients with suspected small-bowel diseases. Endoscopy 2007;39:208-15. |
|
17.
|
Khalife S, Soyer P, Alatawi A, Vahedi K, Hamzi L, Dray X, et al. Obscure gastrointestinal bleeding: preliminary comparison of 64-section CT enteroclysis with video capsule endoscopy. Eur Radiol 2011;21:79-86. |
|
18.
|
Wold PB, Fletcher JG, Johnson CD, Sandborn WJ. Assessment of small bowel Crohn disease: noninvasive peroral CT enterography compared with other imaging methods and endoscopy--feasibility study. Radiology 2003;229:275-81. |
|
19.
|
Paulsen SR, Huprich JE, Fletcher JG, Booya F, Young BM, Fidler JL, et al. CT enterography as a diagnostic tool in evaluating small bowel disorders: review of clinical experience with over 700 cases. Radiographics 2006;26: 641-57. |
|
|
|











