Comparison of the Agitation-Reducing Effects of Esmolol and Lidocaine in Pediatric Strabismus Surgery: A Double-Blind, Randomized Clinical Study
Article information
Abstract
Objective
Agitation is a common symptom in children undergoing surgery, especially when surgeries are performed under sevoflurane and when patients undergo strabismus surgery. Because agitation can increase the risk of falls and lacerations on surgical sites and can delay discharge from the recovery room, adopting measures to reduce the incidence of agitation is essential. This study aimed to compare the agitation-reducing effects of lidocaine and esmolol administered individually or as a combination.
Methods
We included 80 patients scheduled to undergo strabismus surgery. Thiopental and sevoflurane were administered to induce general anesthesia. Group EL received lidocaine (2 mg/kg) right after the end of surgery and esmolol (0.5 mg/kg) immediately after recovery from anesthesia after turning the anesthetic gas off; group L received lidocaine at 2 mg/kg right after the end of surgery and did not receive esmolol, group E did not receive lidocaine at the end of the surgery but received esmolol at 0.5 mg/kg right after recovery from anesthesia, and group C received neither esmolol nor lidocaine. Agitation severity was assessed using the objective pain score, Pediatric Anesthesia Emergence Delirium Scale immediately after recovery from anesthesia and until discharge from the recovery room.
Results
Groups L and EL showed significantly lower agitation than groups E and C right after recovery from anesthesia, right after arrival to the recovery room, and 10 minutes after arrival to the recovery room (P<0.05). Groups L and EL showed no differences in the reduction of the severity of agitation (P>0.05).
Conclusion
Compared to the groups without lidocaine administration, groups L and EL, which received 2 mg/kg lidocaine, showed a higher level of reduction in agitation immediately after recovery from anesthesia and right after arrival to the recovery room (P<0.05).
INTRODUCTION
Emergence delirium (ED) is a state of perceptual confusion with psychological and physical agitation that occurs when waking up from anesthesia [1]. It is commonly observed in children, with a reported incidence of 10%–80% [2]. In particular, strabismus surgery is known to be associated with a high incidence of agitation [3]. Despite the advantages of sevoflurane, an inhalational anesthetic commonly used in children, in reducing airway irritation and ensuring faster awakening [4], this anesthetic is known to aggravate agitation in children due to the rapid removal of residual gas caused by low lipid solubility [5] and the increased release of noradrenaline in the preoptic area [6]. Although agitation is alleviated over time, it increases the risk of injury during the onset of symptoms and the length of hospital stay due to sequelae, highlighting the need to urgently identify measures to prevent or alleviate [7].
Many drugs have been used to prevent agitation or reduce the severity of relevant symptoms and are currently being investigated [8,9]. In general, lidocaine is known to reduce cough or sore throat [10] or cerebral hemodynamic changes after tracheal intubation and is also known to be effective in neuropathic pain [11]. Moreover, one study also reported that when intravenous lidocaine was used alone, agitation in children was rapidly alleviated [12]. Esmolol is an ultra-short-acting beta-blocker, and it has been shown to play a pivotal role in reducing heart rate (HR). It also acts on the central nerves to induce central analgesic effects [13] and reduces postoperative nausea and vomiting (PONV) [14]. Although their mechanism of action is not certainly defined, beta receptor blockers have also been reported to reduce physical and electroencephalogram activity in animals [15]. Esmolol is also known to decrease the consumption of propofol and sevoflurane doses [16]. Therefore, based on the results of studies reporting that lidocaine can help reduce postoperative cough and agitation [12,17] and studies reporting that esmolol monotherapy can alleviate agitation due to its sparing effect and mechanism of action [15,16], this study aimed to investigate the agitation-reducing effects of lidocaine and esmolol when administered alone or in combination.
MATERIALS AND METHODS
1. Study design and patients
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board and Human Research Ethics Committee of Soonchunhyang University Cheonan Hospital (IRB number: 2018-11-016; approved date: 2019. 1. 8) and Clinical Research Information Service (number: KCT0008195 on 16 February 2023).
A total of 100 pediatric patients aged 5–9 years who were scheduled to undergo unilateral strabismus surgery were identified to participate in this study. The exclusion criteria were as follows: (1) patients who had undergone bilateral strabismus surgery because the eye contact for these patients could not be assessed using the Pediatric Anesthesia Emergence Delirium (PAED) Scale (Table 1), which is an agitation scale; (2) patients with mental illness (such as excessive anxiety) or cardiac or respiratory disease; (3) those that had adverse reactions to lidocaine or esmolol; (4) patients who were excessively unstable before surgery or had a low HR, fever, cough, or persistent tachycardia and had to receive perioperative esmolol continuously during surgery; and (5) those whose guardians did not consent for them to participate in the study. Finally, 20 patients were excluded from the study. Of the remaining 80 patients, 20 were assigned to each of the four groups using a random group generator program (Fig. 1). Patients in group EL received esmolol (0.5 mg/kg)+ lidocaine (2 mg/kg); those in group E received esmolol (0.5 mg/kg); those in group L received lidocaine (2 mg/kg); and those in group C received normal saline. Before going into surgery, the research was explained to the patients and their parents, and written informed consent was obtained from the parents/guardians.
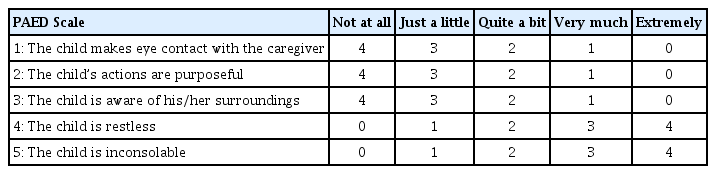
The Pediatric Anesthesia Emergence Delirium Scale

Flow diagram.
2. Intervention and blinding
Anesthesia was induced by thiopental sodium (5 mg/kg) and maintained using one minimum alveolar concentration of sevoflurane. Intubation was performed through a polyvinyl chloride tube to secure an airway, and rocuronium (0.6 mg/kg) was administered to maintain the operation. Air mixed with oxygen (O2) was administered to maintain the fraction of inspired oxygen (FiO2) at 0.5. The tidal volume and respiratory rate were controlled to maintain normocapnia. After the induction of anesthesia, dexamethasone 0.25 mg/kg was administered to the patients before the initiation of surgery to prevent PONV. After surgery, pyridostigmine 0.25 mg/kg and glycopyrrolate 0.1–0.2 mg were used for muscle reversal.
Esmolol or nicardipine administration was planned for patients with increased blood pressure (BP) and HR of ≥25% from baseline, while administration of atropine 0.01 mg/kg was planned for patients with bradycardia. As eye surgery is less likely to cause bleeding and requires a small surgical field, 1:4 saline dextrose fluid was administered at 2 mL/kg/hr for maintenance during surgery. The time of onset of action of lidocaine and esmolol are approximately 2 minutes and 60 seconds, respectively. Therefore, in group EL, lidocaine at 2 mg/kg was administered immediately after surgery, and esmolol at 0.5 mg/kg was administered when the patients demonstrated voluntary movement after switching off the anesthetic gas administration and after HR increased. In group E, a saline volume equivalent to lidocaine at 2 mg/kg was administered to the patients immediately after surgery, and esmolol at 0.5 mg/kg was administered when the patients demonstrated voluntary movement with a rise in HR. In group L, lidocaine at 2 mg/kg was administered to the pediatric patients immediately after surgery, and a saline volume equivalent to esmolol 0.5 mg/kg was administered when the patients demonstrated voluntary movement after switching off the anesthetic gas administration and a rise in HR. In group C, the patients received saline volume equivalent to lidocaine at 2 mg/kg and esmolol at 0.5 mg/kg immediately after surgery and when they demonstrated voluntary movement and rise in HR, respectively. Patients were extubated once they opened their eyes, grimaced, acted intentionally, and had tidal volumes equal to 5 mL/kg during spontaneous breathing. Next, the severity of agitation was accessed using the Objective Pain Scale (OPS) (Table 2) and the PAED Scale (Table 1). Patients with normal oxygen saturation levels, absence of cyanosis, and stable BP and HR were transferred to the recovery room. The OPS and PAED assessments were performed immediately after the patients were transferred to the recovery room and every 10 minutes thereafter; the patients’ vital signs were also measured. If the patients were agitated, the staff tried to calm them down, either verbally or by giving them a hug, and if agitation persisted until 10 minutes after arriving at the post-anesthesia recovery unit, fentanyl 1 μg/kg was administered. The Aldrete score was assessed, and a score ≥9 was required for discharge. The time from arrival to the recovery room to discharge was also recorded.

The Objective Pain Scale
The study was double-blinded by ensuring that the investigator who administered the drugs and performed the assessments was blinded to the allocation of patients. Nurses, who were aware of the group allocation, prepared the drugs and gave them to the investigator. Administration of drugs to the patients and assessment of patient status were conducted by only one investigator.
3. Statistical analysis
IBM SPSS ver. 26.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. The sample size was calculated by calculating the N number based on statistically significant values in a previous study [18]. One-way analysis of variance (ANOVA) and Pearson’s chi-square test were used to assess categorical variables, including age, gender, operation duration, anesthesia duration, extubation time, recovery time, BP, HR, and fentanyl dose. One-way ANOVA and Kruskal-Wallis test were used to assess continuous variables, including the agitation scale scores. A post-hoc test was performed for between-group comparisons. All data were expressed as mean±standard deviation or IQR (median [1Q-3Q interquartile]). P-values <0.05 were considered statistically significant.
RESULTS
The four groups did not show statistically significant differences in patient age (P=0.687), sex (P=0.875), operation duration (P= 0.979), anesthesia duration (P=0.980), extubation time (P=0.578), recovery time (P=0.072), and total dose of fentanyl (P=0.596) (Table 3). Regarding the vital signs measured when the patients recovered from anesthesia, systolic blood pressure (SBP) (119.8± 10.5 mm Hg) and HR (106.2±8.8 beats/min [bpm]) in group E and SBP (113.2±16.2 mm Hg), DBP (73.4±17.4 mm Hg), and HR (108.6±7.6 bpm) in group EL, both of which received esmolol, were significantly lower than those in group C and group L, which did not receive esmolol (Table 4). The patients in group E, who received esmolol alone, showed lower SBP and HR on recovery from anesthesia than those in groups C and L (Table 4). The result demonstrated that the OPS and PAED scores after recovery from anesthesia and right after arrival to the recovery room were significantly lower in groups L and EL than in groups C and E (Tables 5, 6). The patients in group E demonstrated lower SBP and HR on recovery from anesthesia than those in groups C and L (Table 4). Although the vital signs in group E were more stable than those in the other groups, reduced agitation was not observed in group E.
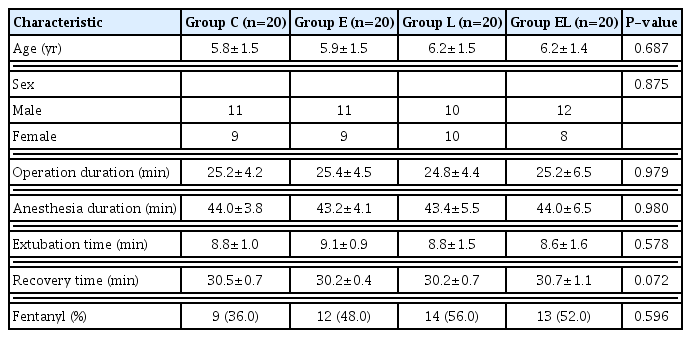
Characteristics of patients

Hemodynamic data of patients
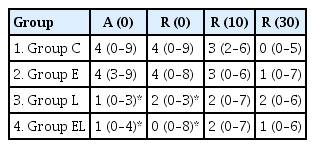
The Objective Pain Score
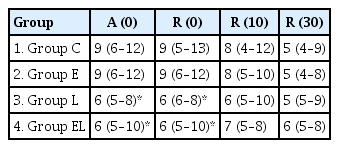
Pediatric anesthesia emergence delirium
DISCUSSION
Herein, we aimed to compare the agitation-reducing effects of lidocaine and esmolol, administered individually or as a combination. We found that groups L and EL, administered with 2 mg/kg lidocaine, showed a higher level of reduction in agitation immediately after recovery from anesthesia and right after arrival to the recovery room compared to the groups that did not receive lidocaine.
Emergence agitation can have clinically significant consequences, such as the requirement of additional treatment or prolongation of hospital stay, and consequently, it cannot be overlooked. The risk factors for agitation include pain, age, eye surgery, and the use of inhalational anesthetics [19]. Sevoflurane is an inhalational anesthetic commonly used to induce anesthesia in children [20–22]; it increases the severity of agitation and the risk of PONV. Despite these disadvantages, sevoflurane is widely used as an inhalational anesthetic worldwide because it reduces airway irritation and has a faster awakening time in pediatric patients [23]. Therefore, this study used sevoflurane to maintain anesthesia.
Several studies have focused on reducing agitation when pediatric patients recover from anesthesia [7,24–26]. Propofol is known to be effective in reducing airway hypersensitivity and PONV in children [27]. One study reported that administering propofol when pediatric patients recover from anesthesia after the end of surgery reduced agitation and prevented them from prolonged hospitalization. Thus, the use of propofol in pediatric surgery is currently increasing [28].
However, propofol administration can also result in unstable vital signs such as bradycardia, tachycardia, hypotension, and hypertension [29]. In particular, the use of small doses of propofol for prophylactic purposes after surgery can cause delayed awakening and complications such as hypoxia due to apnea [30]. Thus, the use of propofol to reduce agitation is associated with some limitations [23]. Dexmedetomidine has also been reported to reduce agitation in pediatric patients [26]. A key adverse effect of dexmedetomidine is bradycardia, which may occur during eye surgery [20]. Despite these risks, dexmedetomidine can be used for other surgeries in pediatric patients. However, we concluded that its use in eye surgery is extremely risky.
Eye surgery can also cause PONV, affecting the onset of agitation [31,32]. Accordingly, to prevent PONV in pediatric patients undergoing eye surgery, a combination of antiemetics—ondansetron and dexamethasone—is used. According to one study, a reduction in PONV also resulted in agitation reduction [33]. Although this study also considered the possibility of administering ondansetron to decrease PONV, it was not used in this study due to concerns about the burden of additional cost and side effects such as Q-T interval prolongation, headache, and dizziness [34]. Lidocaine has been reported to reduce PONV, although the mechanism of action is unknown [35]. However, in this study, no differences were observed in the incidence of nausea or vomiting between groups.
In general, the administration of lidocaine has been reported to reduce postoperative pain, doses of analgesic drugs, length of hospital stay, and degree of cerebral hemodynamic changes at airway manipulation has been shown effective in reducing airway hypersensitivity [11]. Pediatric patients show a higher risk of airway obstruction after postoperative extubation due to airway hypersensitivity [36]; agitation can be aggravated by complications such as hypoxia. We anticipated lidocaine administration as a bolus before extubation could reduce airway irritation and effectively prevent agitation.
In one study, intravenous lidocaine administration at 1.5 mg/kg before extubation was shown to be effective in reducing hemodynamic irritation and sore throat [37]. However, another study reported that 1.5 mg/kg of lidocaine did not prevent agitation [38]. A previous study showed that when 1.5 mg/kg lidocaine was administered alone, agitation in children did not reduce [39]. Therefore, based on one study reporting that the administration of lidocaine (2 mg/kg) effectively reduced agitation [12], we set the lidocaine dose at 2 mg/kg in our study. The group receiving lidocaine at 2 mg/kg alone showed reduced agitation from the end of the surgery until 10 minutes after arrival to the recovery room compared to the control group, and no patients complained about postoperative lidocaine-related side effects. The results of previous studies suggest that the reduction of agitation varies depending on the doses [12,38].
As esmolol delays the metabolism of inhaled agents or lidocaine by reducing cardiac output, we expected it to show synergistic effects with other drugs [40]. As per our findings, administration of a (single) bolus dose (0.5 mg/kg) did not lead to reduced agitation. However, we expect higher bolus doses or the use of extra infusion to reduce agitation because anxiety, pain, and sympathetic activation are causes of agitation [5]. Furthermore, one study reported that esmolol reduced postoperative pain and sympathetic activation [41]. However, similar to dexmedetomidine, esmolol can cause severe bradycardia in patients undergoing eye surgery; therefore, we concluded that additional infusion of esmolol in the case of eye surgery is risky and did not use it in this study. In group E, esmolol was administered once the anesthetic drug was turned off and the patient had awakened; hence, the HR and SBP decreased more than those in other groups that did not receive esmolol. Despite this, agitation was not reduced. Consequently, whether a transient reduction in BP or HR is associated with the reduction in agitation remains unclear.
In previous study since there was no group administered with esmolol alone, the degree of hemodynamic change and the effects of esmolol administration to reduce agitation were unknown [39]. The effectiveness in the lidocaine and esmolol combination group is thought to be due to the synergistic effect of the two drugs; however, it was necessary to further study the degree of change in agitation according to the difference in drug dosage. Moreover, because there was a limitation of not using PAED, one of the scales for measuring agitation in children, this present study used PAED.
Fentanyl is a short-acting opioid analgesic [42] and has been widely used to ease agitation in pediatric patients [43]. The doses used to reduce agitation vary across studies, ranging from 1 to 3 μg/kg [43]; Herein, we used doses up to 1 μg/kg. However, none of the patients showed agitation requiring additional use of fentanyl. PONV is a complication of eye surgery [44] and can be worsened by fentanyl. Therefore, we considered administering ketorolac instead of fentanyl. However, since pain after eye surgery is not severe [45], and ketorolac has been reported to have no effect in reducing agitation [46], we used fentanyl. Fortunately, the frequency of PONV was not high in all four groups, and all four groups showed no differences in the incidence of nausea and vomiting after receiving fentanyl.
1. Limitations
First, as this study included only those patients who had undergone unilateral eye surgery, objective evaluation of the severity of agitation may not have been entirely possible owing to the reduced visual disturbance. However, we expected that agitation would occur even in unilateral eye surgery because agitation can be attributed to many causes other than visual disturbances [2]. Second, lidocaine and esmolol were infused in two other studies during surgery [47,48]. However, since only one bolus injection was used at the end of the surgery in this study, it may have had a limited effect in reducing agitation. This study did not use an infusion of esmolol, as it may increase the risk of bradycardia [49]. In general, strabismus surgery usually does not cause much pain [45]. Thus, even alleviating temporary agitation early after awakening from anesthesia was considered meaningful. Moreover, an increased dose of lidocaine can cause side effects, and when it is used for pediatric patients, the risks are aggravated because pediatric patients cannot express their symptoms. So, in this study, a single lidocaine bolus dose, with no additional infusion, was used.
2. Conclusions
Administration of lidocaine at 2 mg/kg immediately after the end of the surgery was effective in reducing agitation from the time when the pediatric patients recovered from anesthesia until 10 minutes after arrival to the recovery room. Therefore, lidocaine dose influenced the severity and duration of agitation. Accordingly, additional studies are required to investigate the use of lidocaine infusion or high doses of lidocaine for strabismus surgery and other surgical procedures.
ACKNOWLEDGMENTS
This work was supported by the Soonchunhyang University Research Fund for financial support (No. 2023-001).
Notes
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: JYJ, KKS. Methodology: JYJ, JSP. Data curation: JYJ. Software: JYJ, HSJ. Validation: YHS. Investigation: JYJ, HSJ. Resources: HRC. Writing–original draft preparation: JYJ. Writing–review and editing: WJK, JMA. Visualization: YJP, YES. Supervision: KSK. Project administration: JYJ. Funding acquisition: JYJ. All authors have read and agreed to the published version of the manuscript.