병리학적으로 확진된 유방의 고에코 종괴에서 악성과 양성의 감별점
Pathologically Proven Hyperechoic Masses of the Breast on Ultrasound: Differentiation of Malignant and Benign Lesions
Article information
Trans Abstract
Objective:
The aim of this study was to evaluate the frequency of the characteristic sonographic findings of the pathologically confirmed hyperechoic masses on breast ultrasonography, and clinical and sonographic findings in differentiating the malignant from benign hyperechoic masses.
Methods:
One hundred and ninety hyperechoic masses on breast ultrasonogram of which were pathologically confirmed were retrospectively analyzed. The clinical features were reviewed according to patient’s age, size of mass, and palpability. The sonographic features were reviewed according to the Breast Imaging Reporting and Data System 4th lexicon: margin, orientation, shaped, and posterior acoustic features. The sonographic features of the benign and malignant masses were statistically analyzed using the chisquare test, the Fisher’s exact test, and T-test.
Results:
The benign masses were 42 cases (79.2%) and the malignant masses were 11 cases (20.8%). Patient age, size of mass, palpability were not significant difference between malignant and benign masses (P=0.684, P=0.377, P=0.746). Mixed hyperechoic, noncircumscribed margin, irregular shape, nonparallel orientation were significantly different for malignant and benign masses (P<0.001, P=0.01, P=0.003, P=0.025). But posterior acoustic features were not statistically different for malignant and benign masses.
Conclusion:
Malignant masses with hyperechogenicity were more likely than benign masses to have mixed hyperechoic, noncircumscribed margin, irregular shape, nonparallel orientation. Therefore, pathologically confirm should be performed hyperechoic masses with suspicious findings.
서 론
유방초음파는 유방촬영술과 함께 유방종괴의 진단에 중요한 검사방법으로 사용되고 있으며 유방종괴의 특징을 평가하는데 유용하다. 유방종괴의 분석에서 에코패턴은 양성과 악성을 구분하는데 사용되는 기술어(descriptor)로 일반적으로 유방암은 저에코를 보이는 것으로 알려져 있다[1,2]. 고에코로 보이는 종괴는 양성을 시사하는 소견으로 알려져 있으나 고에코를 보이는 악성 병변에 대한 보고가 드물게 있어 고에코에 대한 평가는 아직도 이견을 보인다[3- 11].
Stavros 등[1]은 초음파에서 발견된 750예 종괴를 대상으로 한 연구에서 42예의 심한 고에코 종괴 중 악성은 없었고 고에코는 악성에 대한 높은 음성 예측도(100%)를 갖는 양성소견이라고 보고하였다. 다른 연구에서도 고에코 종괴 중 악성 종괴는 없다고 보고하였 으나 적은 개체 수에 대한 연구였다[12,13].
그러나 몇몇 연구에서는 적은 수이긴 하지만 고에코를 보인 유방암에 대해 보고를 하고 있으며 침윤성 소엽암(infiltrative lobular carcinoma), 침윤성 관상피암, 관내 유두상암(intraductal papillary carcinoma), 림프암, 혈관육종, 전이암 등에서 고에코를 보인다고 하였다[3-11]. 이러한 연구들은 고에코 종괴가 반드시 양성은 아니며 악성을 배제할 수 있는 소견이라는 기존의 주장과 다른 결과이다. 본 연구는 병리학적으로 확진된 유방의 고에코 종괴에서 양성과 악성 종괴의 빈도를 알아보고 두 종괴 간의 임상소견과 초음파소견을 분석하여 양성과 악성 종괴를 구분하는데 있어 통계적으로 유의한 차이가 있는지를 알아보고자 하였다.
대상 및 방법
2005년 12월부터 2011년 6월까지 순천향대학교 천안병원에서 유방초음파검사를 시행한 환자들 중 전자의무기록(medical record data base)에서 검색을 통하여 고에코 종괴를 가진 것으로 나타난 190명 중에서 병리학적으로 확진된 53명의 53예를 후향적으로 분석하였다. 병리학적 확진은 중심부 바늘생검(n=30), 진공보조 중심부 바늘생검(맘모톰, n=6), 외과적 절제생검(n=12), 수술(n=5)을 통해 시행되었다.
중심부 바늘생검은 모두 초음파 유도하에 14게이지 코어바늘을 이용하여 각 병소당 최소한 4개 이상의 조직을 얻었으며 진공보조 중심부 바늘생검(맘모톰)은 8게이지 코어바늘을 이용하여 시행하였다. 수술적 방법은 종괴절제술(lumpectomy) 2예, 단순 유방절제술(simple mastectomy) 1예, 피부보존 유방절제술(skin sparing mastectomy) 1예, 변형 근치적 유방절제술(modified radical mastectomy) 1예였다. 환자에 따라 중심부 바늘생검과 절제생검 또는 중심부 바늘생검과 수술을 중복으로 시행한 경우도 있었다. 중심부 바늘생검과 진공보조 중심부 바늘생검을 같이 시행한 경우는 3 예, 중심부 바늘생검과 외과적 절제생검을 같이 시행한 경우는 4 예, 중심부 바늘생검과 수술을 같이 시행한 경우는 5예였다. 병리학적 확진을 시행하지 않은 137명 중 79명은 2년 이상의 추적검사에서 변화가 없었으며, 37명은 1년 후 추적검사에서 변화가 없었고 나머지 21명은 추적검사를 시행하지 못하였으며, 추적검사 중 악성으로 발전한 예는 없었다.
유방초음파검사는 5-17 MHz 고해상력 선형탐촉자(iU 22; Philips Medical System, Bothell, WA, USA)와 5-12 MHz 고해상력 선형탐촉자(HDI 5000; Philips Medical System)를 사용하였다. 초음파는 기본적인 횡단 주사와 종단 주사를 사용하였고, 유선과의 관계를 잘 보기 위해 방사상 주사를 보완적으로 사용하였다.
임상소견으로 환자의 나이와 종괴의 크기, 촉지(palpability) 유무에 대해 분석하였다. 환자의 의무기록을 통해 나이와 촉지 유무를 기록하였고, 종괴의 크기는 초음파에서 전자 자로 횡단경과 종단경을 측정하여 더 긴 길이로 기록하였다.
영상분석은 의무기록에서 고에코로 보인 환자들에 대하여 병리학적 결과에 대한 정보 없이 초음파영상을 후향적으로 분석하였다. 종괴의 에코패턴은 초음파에서 유방의 피하지방과 비교하여 상대적으로 증가된 에코를 보일 때를 고에코(hyperechoic) 종괴로 보았고 종괴의 고에코 부분이 균일하게 증가된 경우 균일 고에코(homogeneous hyperechoic)로, 종괴의 고에코 부분이 50% 또는 그 이상에서 보이나 고에코가 아닌 부분이 혼합되어 있을 때를 혼합성 고에코(mixed hyperechoic)로 정의하였다.
모든 병변은 American College of Radiology의 Breast Imaging Reporting and Data System 4판의 lexicon에 따라 병변의 변연, 모양, 방향성, 후방에코소견에 대해 분석하였다. 변연은 국한성(circumscribed) 과 비국한성(noncircumscribed)으로, 모양은 난원형 (oval) 또는 원형(round)과 불규칙형(irregular)으로, 방향성은 평행(parellel)과 비평행(non-parellel)으로, 후방에코소견은 무후방 음향소견(no posterior acoustic features), 후방음향 증강(posterior acoustic enhancement) 또는 후방음영(posterior shadowing)에 대해 분석하였다.
최종 병리학적 결과에 따라 양성과 악성 종괴군으로 나누었고 두 군 사이에 임상소견과 초음파소견의 각각의 항목에 대해 유의한 차이가 있는지 통계학적 분석을 시행하였다. 임상소견 중 환자의 나이와 종괴의 크기는 T-검정을 사용하였고 촉지 여부는 Fisher’s test를 통해 분석하였다. 초음파소견 중 에코패턴은 카이제곱검정법(chi-square test)을 통해 분석하였고 변연과 모양, 방향성, 후방음 향소견은 Fisher’s exact test를 통해 분석하였다. P값이 0.05 이하일 때 통계적으로 유의한 것으로 보았다. 통계학적 분석은 SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA)을 사용하였다.
결 과
53예 종괴 중 양성은 42예(79.2%)이고 악성은 11예(20.8%)였다. 양성 종괴 중 섬유낭종성 변화(fibrocystic change)가 15예로 가장 많았고 섬유선종(fibroadenoma) 9예, 지방종(lipoma) 7예, 지방괴사(fat necrosis) 5예, 정상 유방조직(breast tissue) 2예였으며, 혈관지방종(angiolipoma), 모기질종(pilomatrixoma)과 만성 육아종성 유선염(chronic granulomatous mastitis)은 각각 1예였다. 악성 종괴는 점액암(mucinous carcinoma) 4예, 침윤성 관상피암(infiltrative ductal carcinoma) 3예, 관상피내암(ductal carcinoma in situ) 3 예, 미만성 거대 B세포 림프암(diffuse large B cell lymphoma)이 1 예였다(Table 1).

Classification of pathologically confirmed 53 hyperechoic masses
환자들의 연령은 17세에서 82세였고, 종괴의 크기는 0.5 cm에서 9 cm 사이로 평균 2.1 cm이었다. 양성 종괴군의 연령은 17세에서 82 세였고, 종괴의 크기는 0.5 cm에서 9 cm 사이로 평균 2.1 cm이었다. 악성 종괴군의 연령은 34세에서 66세 사이, 종괴의 크기는 0.6 cm 에서 7 cm 사이로 평균 2.3 cm이었다. 촉지되는 종괴 중에서 양성 종괴는 23예(54.8%)였고, 악성 종괴는 7예(63.6%)였다. 임상소견에 대한 통계적 분석에서 환자의 연령과 종괴의 크기, 촉지 여부는 두 군 사이에 유의한 차이가 없었다(P= 0.377, P= 0.684, P= 0.746) (Table 2).

Clinical and sonographic features of 53 hyperechoic masses
양성 종괴 중 균일 고에코를 보인 종괴는 25예였고 혼합성 고에코를 보인 종괴는 17예였다. 변연은 국한성 변연이 17예, 비국한성 변연이 25예였다. 모양은 40예에서 타원형 또는 원형을 보였고, 2예에서 불규칙형을 보였다. 방향성은 평행한 방향성이 41예에서 보였고 비평행한 방향성은 1예에서만 보였다. 후방음향에 대한 분석에서는 후방음영을 보이지 않는 경우가 25예, 후방음영을 보이는 경우가 5예에서 후방음영의 증강을 보이는 경우가 12예였다(Table 2, Figs. 1-5).
Fibrocystic change in 41-year-old woman. Ultrasonogram shows a circumscribed oval homogeneous hyperechoic mass (arrows) in the right breast.

Hamartoma in 43-year-old woman with palpable mass. (A) Mammogram shows a partly obscured oval isodense mass (arrows) in the right breast. (B) Ultrasonogram shows a circumscribed oval mixed hyperechoic mass (arrows) in the right breast.
악성 종괴는 11예 모두 혼합성 고에코를 보였으며, 균일 고에코를 보인 예는 없었다. 변연은 모두 비국한성 변연을 보였고 그 중 불분 명한 변연(indistinct)은 6예, 미세소엽형 변연(microlobuated)은 3예, 각진형 변연(angular)은 2예였다. 모양은 원형 또는 타원형이 6예, 불규칙형은 5예에서 보였다. 방향성은 평행한 방향성을 보인 예가 8예였고, 비평행한 방향성을 보인 예가 3예였다. 후방음영은 후 방음영이 보이지 않는 경우가 6예, 후방음영이 보이는 경우가 1예, 후방음향의 증강은 4예였다(Tables 2, 3, Figs. 6, 7). 양성과 악성 종괴의 초음파소견 중 에코패턴(P<0.001)과 변연(P= 0.01), 모양(P= 0.003), 방향성(P= 0.025)이 통계적으로 유의한 차이를 보였고 악성 종괴에서 양성 종괴보다 혼합성 고에코패턴, 비국한성 변연, 불규칙형 모양, 비평행한 방향성이 흔히 보였다. 반면에 종괴의 후방 음향소견(P= 0.273)은 두 군 사이에 유의한 차이가 없었다(Table 2).
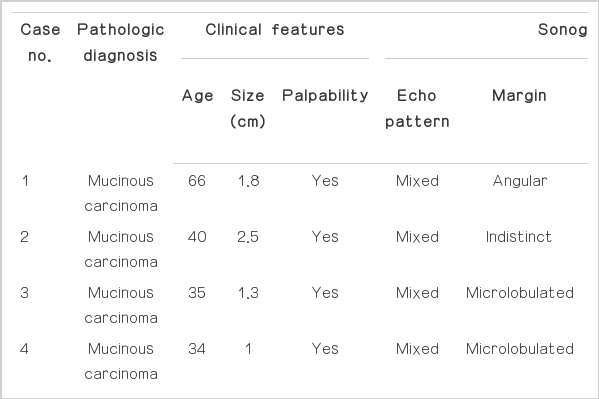
Clinical and sonographic features of 11 malignant hyperechoic masses

Invasive ductal carcinoma in 46-year-old woman with palpable mass. (A, B) Ultrasonograms show an indistinct relatively round mixed hyperechoic mass (arrows) in the left breast.
Diffuse large B cell lymphoma in 43-year-old woman with palpable mass. (A, B) Mammograms show a partly obscured oval isodense mass (arrows) in the right breast. (C) Ultrasonogram shows a partly indistinct oval mixed hyperechoic mass (arrows) in the right breast.
고 찰
유방초음파에서 고에코 종괴는 양성을 시사하는 소견으로 알려져 있다. 그러나 몇몇 연구에서는 고에코 종괴로 보이는 유방암을 보고하고 있다. Soon 등[10]은 393예 유방암선별검사(screen detected breast cancer)에서 2예(0.5%)의 고에코 종괴를 보고하였고, 고에코 유방암과 저에코 유방암의 비가 1:180이라고 하였다. Skaane과 Engedal [11]은 194예 침윤성 관상피암에서 4예(2%)의 고에코 종괴를 보고하였다. Linda 등[4]에 의하면 1,849예 악성 종괴 중 9예(0.4%)가 고에코를 보였고 이들 종괴는 침윤성 소엽암, 침윤성 관상피암, 관내 유두상암이었다. 이러한 연구들은 고에코 종괴가 반드시 양성은 아니며 악성인 경우도 있다는 결과를 보여주는 연구들로 고에코가 악성을 배제할 수 있는 소견이라는 기존의 주장과 다른 결과이다.
본 연구에서도 병리학으로 확진된 53예 고에코 종괴 중에서 11예 (19.9%)가 악성으로 확인되었다. 본 연구는 다른 악성 고에코 종괴의 연구들보다 높은 악성의 비율을 보이는데 이는 아마도 병리학적으로 확진된 종괴만을 대상으로 연구를 진행하였기 때문으로 생각 된다. 유방의 고에코 종괴는 일반적으로 양성 종괴로 알려져 있기 때문에 이러한 양성 종괴는 병리학적 확진이 필요하지 않고 추적관찰을 하며 지켜보는 것이 일반적이다. 본 연구의 대상인 53예의 고에코 종괴들은 에코패턴을 제외한 다른 소견 중에서 초음파적 악성 의심소견이 있어 병리학적 확진을 시행하였다. 따라서 다른 연구들보다 악성의 비율이 상대적으로 높은 것으로 생각된다.
본 연구에서는 혼합성 고에코와 비국한성 변연, 불규칙형 모양, 비평행한 방향성이 악성 종괴에서 의미 있게 더 높은 빈도를 보였다. Linda 등[4]의 연구에서도 병리학적으로 확진된 25개의 고에코 종괴들 중에서 악성과 양성 종괴의 초음파소견을 비교했을 때 악성 종괴에서 비국한성 변연과 비평행한 방향성이 의미 있게 더 높게 나타났다. 또한 통계학적 차이는 보이지 않았으나, 악성 종괴 중에서 내부에 저에코 부분을 포함하는 고에코 종괴가 더 많다고 보고하였다. 즉 악성 종괴에서 균일한 고에코패턴보다 혼합성 고에코 패턴이 더 많았다는 의미로, 본 연구에서도 악성 종괴에서 혼합성 고에코가 100%로 나타났고 양성 종괴보다 통계학적으로 높은 빈도를 보였다.
또한 악성 종괴에서 더 흔하게 보인 비국한성 변연, 불규칙형 모양, 비평행한 방향성은 다른 연구에서도 악성을 시사하는 소견으로 알려져 있다. Starvros 등[1]의 연구에서 침상형 또는 각진형과 같은 비국한성 경계가 악성 종괴에서 더 흔히 보인다고 하였고 Rahbar 등[14]은 비국한적 경계와 불규칙한 모양, 앞뒤로 긴 모양(taller-than wide)이 악성을 예측할 수 있는 소견이라고 보고하고 있다. 따라서 고에코를 보이는 병변일지라도 악성을 시사하는 소견이 있다면 병리학적 확진을 통해 악성을 배제할 필요가 있다. 반면에 종괴의 후방 음영이 악성을 시사하는 소견 중 하나라고 보고하고 있는데[1] 본 연 구에서는 양성과 악성 종괴에서 의미 있는 차이는 보이지 않았다.
고에코 종괴는 발표된 논문마다 조금씩 다른 기준이 적용되었는데 본 연구에서는 고에코 종괴는 피하지방과 비교했을 때 더 높은 에코를 보이는 종괴로 정의하였다. 이러한 고에코는 지방, 혈관, 간질 섬유화, 부종, 가스, 칼슘 등과 단단하게 뭉쳐진 암세포들에 의해 보이는 것으로 알려져 있다. 또한 사상형 양상, 관상 구조물, 암세포의 고형 소와 경성 양상과 같은 세포충실성의 암 불균질성도 고에코패턴에 중요한 영향을 끼친다[15]. 본 연구에서는 고에코를 보이는 양성 종괴로는 섬유낭종성 변화, 섬유선종, 지방종, 지방괴사, 유방조직, 과오종, 혈관지방종, 지질모세포종과 만성육아종이 있었다. 본 연구에 포함된 고에코를 보이는 악성 유방 병변으로는 점액암, 침윤성 관상피암, 관상피내암, 미만성 거대 B세포 림프종이었고 그 외 침윤성 소엽암, 혈관육종, 전이암 등과 같은 악성 병변이 고에코로 보일 수 있다[9,16-18].
본 연구의 제한점은 전자의무기록에서 고에코 종괴를 검색하여 찾았고, 이 중 병리학적으로 확진된 종괴만을 대상으로 후향적 분석을 시행했다는 점이다. 연구의 대상을 초음파검사영상이 아니라 전자의무기록에서 판독소견에 의존하여 대상을 우선 선택했고, 고에코를 보인 모든 종괴를 대상으로 하지 않고 병리학적으로 확진된 종괴만을 대상으로 연구를 시행하였기 때문에 선택 바이어스(selection bias)가 발생할 수 있다. 유방초음파에서 고에코는 양성을 시사하는 소견으로 알려져 있는데, 본 연구에서 고에코 종괴임에도 불구하고 병리학적 확진을 시행한 경우는 환자가 만져지거나 통증 등의 증상이 있거나 불안하여 제거를 원했거나 주치의가 병리학적 확진이 필요하다고 한 8예의 병변을 제외하면 불규칙한 모양, 비국한성 변연과 같은 악성 의심소견을 동반한 경우이다. 따라서 53예의 종괴는 대부분이 악성 의심소견을 갖고 있으며 이러한 사실은 본 연구에서 양성군임에도 불구하고 비국한성 변연, 불규칙 모양과 같은 악성 의심소견의 비율이 높았다는 점을 설명할 수 있을 것이다.
결론적으로, 유방의 코에코 종괴는 반드시 양성 종괴를 의미하는 초음파소견이 아니며 유방초음파의 다른 소견을 같이 고려하여 감별하여야 한다. 고에코 종괴 중에서 혼합성 고에코를 보이거나 비국한성 변연, 불규칙한 모양, 평행하지 않은 방향성은 악성 종괴를 시사하는 소견이며 초음파검사에서 이러한 소견을 보인다면 악성을 배제하기 위해 병리학적 확진이 필요하다.

Fibroadenoma in 37-year-old woman with palpable mass. Ultrasonogram shows a circumscribed oval mixed hyperechoic mass (arrows) in the right breast.
Lipoma in 53-year-old woman with palpable mass. Ultrasonogram shows a circumscribed oval homogeneous hyperechoic mass (arrows) in the right breast.

Fat necrosis in 82-year-old woman with palpable mass. Ultrasonogram shows an indistinct oval homogeneous hyperechoic mass (arrows) with internal hypoechoic portions (arrowheads) in the left breast.