INTRODUCTION
Although the incidence of ischemic stroke in asymptomatic patients with carotid stenosis is low, the incidence of perioperative stroke in patients with carotid stenosis is 36 times that of healthy individuals [1]. Therefore, it is important to maintain cerebral blood flow and oxygenation during anesthesia in patients with carotid artery stenosis, and events that affect cerebral blood flow, such as hypoxia and hypotension, should be prevented. Monitoring of cerebral oxygen saturation through regional cerebral oxygen saturation (rSO2) measurement is useful for detecting changes in cerebral blood flow during surgery. However, for anesthesia of patients with various underlying diseases, it is necessary not only to assess each disease individually but also to evaluate comprehensive physical status, and optimal management should be provided. Here, we report a case of anesthetic management in a patient with left internal carotid artery occlusion and penetrating aortic ulcer (PAU).
CASE REPORT
A 76-year-old female (152 cm, 63 kg, American Society of Anesthesiologists status III) was admitted for elective posterior decompression of L1–3, corpectomy of L2, and posterolateral fixation of T12–L3 for a compression fracture of L2. Her past medical history included high blood pressure and total occlusion of the left internal carotid artery, which was being treated with angiotensin receptor blockers, calcium channel blockers, diuretics, and aspirin. Preoperative laboratory tests showed no abnormal results, but left ventricular (LV) hypertrophy was observed in electrocardiography. Preoperative transthoracic echocardiography revealed concentric LV remodeling and relaxation abnormality of the LV filling pattern (E/E’=18.4), with an ejection fraction of 56%.
Magnetic resonance imaging of the brain and femoral carotid angiography were performed to assess the patient’s perioperative risk. Total left artery occlusion and collateral blood flow were observed (Fig. 1). Furthermore, during femoral carotid angiography, residual contrast agent was detected around the innominate artery, suggesting the possibility of aortic dissection. Thus, aortic dissection computed tomography (CT) was additionally performed for differential diagnosis. A PAU with approximately 14 mm of length and 8 mm of depth of the distal aortic arch and severe calcification with plaque of the innominate artery were revealed (Fig. 2). The cardiovascular surgeon who reviewed these abnormal findings recommended maintaining the perioperative systolic blood pressure below 130 mm Hg.
Upon arrival at the operating room, standard monitors, including a noninvasive blood pressure monitor, three-lead electrocardiography, pulse oximetry, and a bispectral index (BIS) monitor, were attached to the patient. Then, a cerebral oximeter (rSO2, INVOS Cerebral/Somatic Oximeter; Covidien-Medtronic, Boulder, CO, USA) was attached for continuous monitoring of rSO2. General anesthesia was induced with intravenous lidocaine (40 mg), 2% propofol, and remifentanil. Propofol and remifentanil were administered via infusion pump (Agilia; Fresenius Kabi, Bad Homburg, Germany), using the Marsh pharmacokinetic model and Minto model, respectively.
Esmolol (20 mg) was intravenously administered to prevent sudden change of blood pressure and heart rate before endotracheal intubation. After anesthetic induction, a 22G catheter was inserted into the left radial artery, and then the FloTrac/Vigileo system (Edwards Lifesciences, Irvine, CA, USA) was used for continuous monitoring of arterial blood pressure, cardiac output, and stroke volume. A central venous catheter was subsequently inserted into the right internal jugular vein using ultrasound guidance. Anesthesia was maintained with continuous intravenous administration of propofol, remifentanil, and rocuronium. During anesthesia, we adjusted the target concentrations of propofol and remifentanil to maintain the BIS at 40–60 and set up the mechanical ventilator according to the arterial blood gas analysis findings and end-tidal carbon dioxide levels to maintain mild hypocapnia to prevent the steal phenomenon. In addition, according to the recommendation of the cardiovascular surgeon, esmolol, nicardipine, ephedrine, and phenylephrine were administered intravenously when a decrease or increase in blood pressure was necessary to maintain the target systolic blood pressure below 130 mm Hg. After the operation was completed, the patients’ blood pressure gradually increased as the propofol and remifentanil were stopped. Therefore, intravenous esmolol and nicardipine were administered under careful monitoring of the hemodynamic changes during the anesthetic emergence.
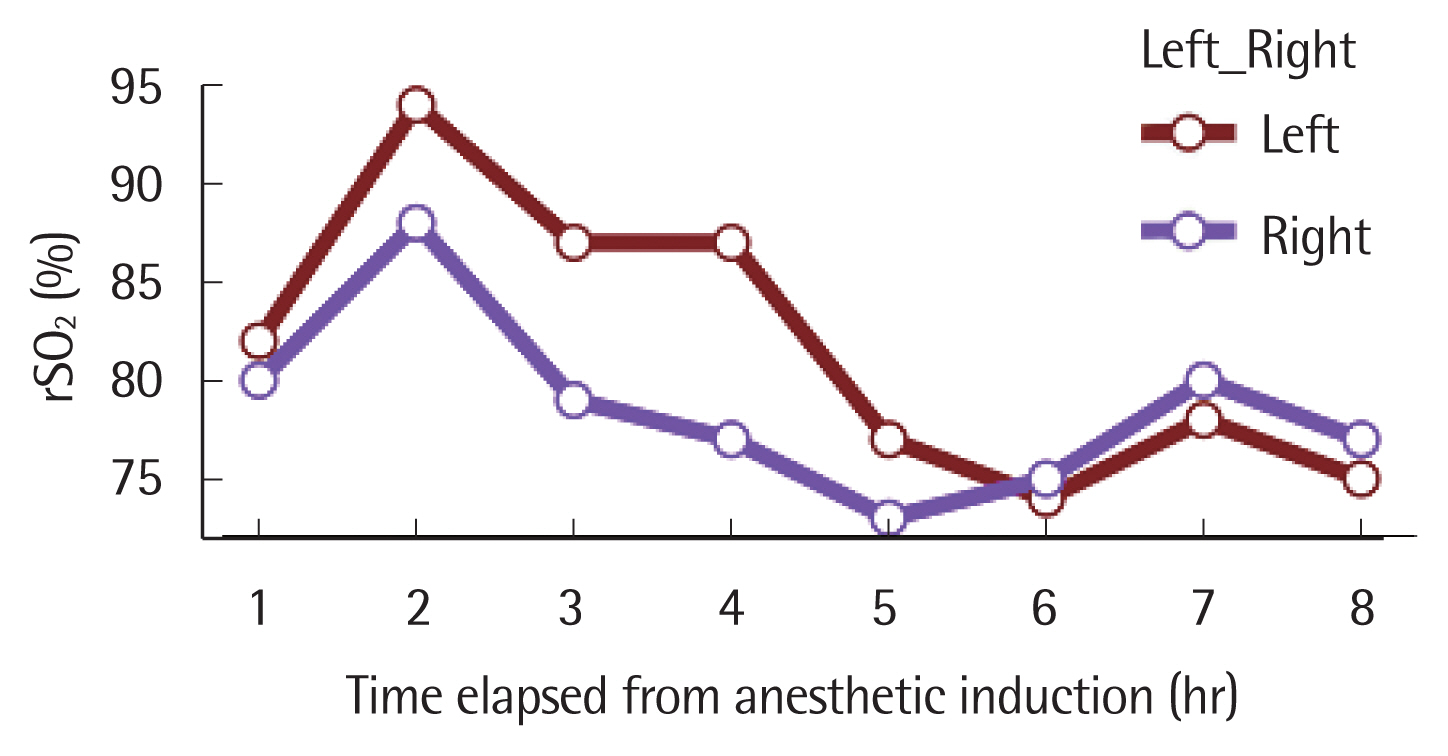
Total anesthesia time was 9 hours and 41 minutes. During the operation, a total of 6 units of packed red blood cells and 6 units of fresh frozen plasma were transfused in the operating room. All hemodynamic parameters were stable, and rSO2 was maintained above 70% (Fig. 3). After the end of surgery, the patient was transferred to the postoperative care unit, where she stayed for 45 minutes, and then was moved to the ward without any immediate postoperative complications.
This study was approved by the institutional review board of Soonchunhyang University Bucheon Hospital (approval no., SCHBC 2021-11-004). The board waived the requirement for patient’ informed consent because this study was a retrospective medical record review.
DISCUSSION
Carotid artery stenosis significantly increases the risk of stroke [1]. The perioperative stroke risk in patients with more than 50% carotid artery stenosis is 3.6%, compared to 0.1% in healthy individuals [2]. According to the literature, the degree of stenosis is most directly related to the factor that increases this stroke risk in asymptomatic carotid stenosis [3]. For patients with carotid artery stenosis, it is important to optimize brain perfusion and minimize myocardial stress [4]. Because intraoperative hypotension can worsen neurological outcomes, proper blood pressure management is required [5]. Several factors are known to decrease cerebral oxygenation during anesthesia. Decreases in cardiac output, changes in blood acid-base status, bleeding, and arterial inflow/venous outflow obstruction induced decreases in cerebral blood flow. In addition, changes in hemoglobin concentration and saturation, pulmonary function, and inhaled oxygen concentrations affect the decrease in oxygen content, which may lead to decreases in cerebral blood flow [6]. These factors can occur at any time during general anesthesia, so the patient should be carefully monitored. For this, the application of monitoring devices that can quantitatively measure rSO2, such as near-infrared spectroscopy (NIRS), may be helpful. [7]. However, due to its low sensitivity and specificity, NIRS should not be used alone in the diagnosis of cerebral ischemia [8].
Our patient had carotid artery stenosis accompanied by PAU discovered incidentally during preoperative workup. Aortic dissection, intramural hematoma, and PAU are considered part of the same spectrum of acute aortic syndrome [9]. PAU is defined as a condition in which ulceration of atherosclerotic plaques in the aorta wall penetrates the media through the intima [10]. There may be no symptoms in the early stages, but as the disease progresses, it can cause intramural hematoma and even life-threatening conditions such as aortic dissection or rupture. The treatment of PAU is determined according to the presence or absence of symptoms and the location of the lesion. For lesions of the descending aorta, if asymptomatic, aggressive antihypertensive medical therapy and regular follow-up can be applied instead of surgical treatment [11]. In our case, conservative treatment and annual CT follow-up were chosen because of the asymptomatic, small lesions in the descending aortic arch.
Therefore, two important considerations in the anesthetic management of this patient were to prevent brain ischemic injury and to prevent acute exacerbation of PAU in the perioperative period. Although the patient had total occlusion of the left internal carotid artery, angiography revealed that sufficient cerebral blood flow was supplied by collateral circulation. To prevent damage to the carotid artery during central venous catheter insertion, the procedure was performed with visualization of the internal jugular vein and carotid artery using ultrasound. Then, continuous rSO2 monitoring was used for the early detection of desaturation. Because the surgery was quite long, there were risks of anemia and hypovolemia following massive hemorrhage and acid–base balance changes. Therefore, cardiac output and volume status were continuously monitored using the FloTrac/Vigileo system. Moreover, we conducted arterial blood gas analysis at regular intervals to obtain arterial oxygen tension, arterial carbon dioxide tension, oxygen saturation, and hemoglobin concentration. To prevent sudden hemodynamic changes due to surgical stimulation, we maintained an appropriate depth of anesthesia via BIS measurement.
In conclusion, for the safe anesthetic management of patients at high risk for complications, it is necessary to predict risk factors in advance through a pre-anesthesia evaluation. During anesthesia, careful patient monitoring is essential, and when complications occur, anesthesiologists need to be prepared to recognize them and respond immediately. In addition, use of appropriate patient-monitoring devices may be helpful in anesthetic management of high-risk patients.