








INTRODUCTION
Since the nasotracheal intubation technique was first suggested by Franz Kuhn in 1902, it has been used for various intraoral and oropharyngeal surgeries [1,2]. However, several complications have been reported. A common complication of this technique is epistaxis. Traumatic avulsion of structures within the nasal cavity has been rarely reported [1,2]. These structural damages often cause massive bleeding or obstruction of the tube. Thus, there have been several studies for safe nasotracheal intubation [1,3,4].
We experienced a case of middle turbinate fracture which showed no immediate signs of fracture such as bleeding or avulsed particles. Two months later, the patient complained of nasal obstruction symptoms and was diagnosed with nasal obstruction from a mass-like lesion originating from the middle turbinate fracture. Symptoms associated with traumatic intubation usually develop during surgery, and it is rare to be found a long time after surgery such as our case. We will report our case, then review the anatomical and technical aspects for safe nasotracheal intubation.
CASE REPORT
A 37-year-old female (height 165 cm, weight 66.8 kg) patient was admitted for transoral approach hemithyroidectomy operation. She had no remarkable medical history but was concerned about keloid scars. The nasotracheal intubation was necessary to secure the surgical field.
Anesthetic induction was achieved with intravenous 1% propofol 120 mg, and rocuronium 50 mg. A 6.0-mm nasal tube (Nasal RAE tracheal tube cuffed; Covidien, Dublin, Ireland) was lubri-cated with sterile gel and gently inserted via the left nostril. Some resistance was encountered, and redirections of the tube were performed several times. No excessive pressure was applied during the intubation. After entering the oropharynx, we guided the tube into the trachea with Magill forceps under the direct vision of the curved Macintosh #3 laryngoscope (Flexicare, Mountain Ash, UK).
There were no remarkable findings and bleedings after the intubation. The operation concluded uneventfully and the patient was discharged from hospital four days after the operation. Two months later, the patient visited and complained of nasal obstruction sensation. Endoscopy and nasal computed tomography revealed a 1.9× 0.9-cm mass abutting the left middle turbinate in the left posterior nasal cavity (Figs. 1, 2). Middle turbinate fracture associated with nasotracheal intubation was diagnosed. She underwent left middle turbinate resection 4 months after the first surgery. The patient provided written informed consent for the publication of clinical details and images.
DISCUSSION
The nasal cavity is positioned above the oral cavity and hard palate and below the skull base. The surface of the nasal cavity comprises pseudostratified columnar epithelium and mucosal stroma which have high vascularity [1,2]. Damage to any part of the whole nasal cavity can result in bleeding because of this high vascularity [1,2].
There are two main anatomical pathways in the nasal cavity for the nasotracheal intubation. The lower pathway lies under the inferior turbinate, and the upper pathway lies between the inferior turbinate and the middle turbinate (Fig. 1). The middle turbinate is part of the ethmoid bone that is attached by a thin lamella to the cribriform plate and highly vascular structure. Any trauma that detaches middle turbinate can result in massive bleeding or cerebrospinal fluid leakage. Hence, the lower pathway is safer passage [1,5]. Judging from the middle turbinate fracture, it seems that the tube was inserted via the upper pathway in this case. Despite no excessive pressure, multiple redirection may cause the middle turbinate fracture. Fortunately, the adjacent skin did not split, and there was no immediate bleeding or signs of fracture.
Fig. 1.
Coronal computed tomography view of the patient: lower pathway (*), upper pathway (★), and the absence of the left middle turbinate bone (☆). Rt, right; Lt, left.
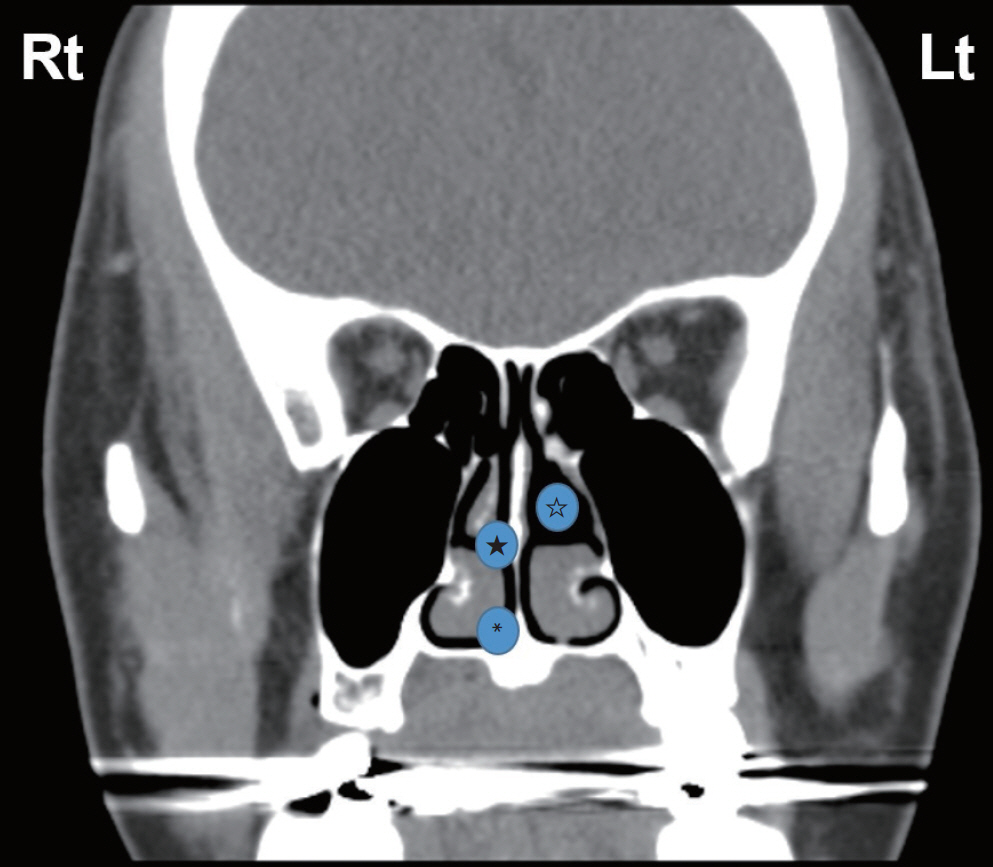
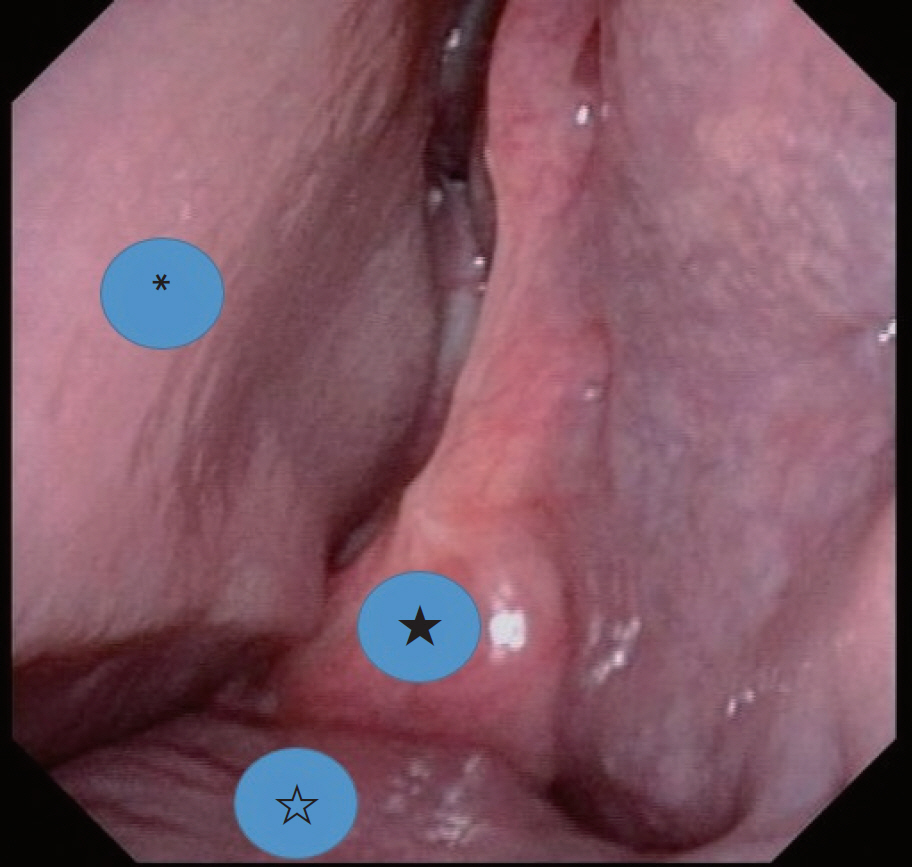
Fig. 2.
Endoscopic image of the patient: nasal septum (*), injured middle turbinate (★), and inferior turbinate (☆).
Traditionally, it is taught that when advancing the nasotracheal tube along the floor of the nostril not to cephalad in the direction of the lower pathway insertion [5]. The common method is that after gently inserting the nasotracheal tube from the nostril to the oropharynx, manipulate the tube into the trachea with Magill forceps under the direct vision by the curved laryngoscope [1,2]. We also used this method in this case.
Many techniques for reducing complications have been reported. Kim et al. [6] reported that thermosoftening of the nasotracheal tube with warm saline significantly reduced epistaxis and nasal damage. Boku et al. [7] suggested that inserting the nasotracheal tube through the right nostril rather than the left results in less epistaxis and decreased intubation time. The possible reason is ex-plained with a left beveled nasotracheal tube (most common type) and the routine left-handed laryngoscopy manipulation is mechanically advantageous when the tube is placed on the right side of the oropharynx [7,8].
Inserting an esophageal stethoscope into the Murphy-tipped nasotracheal tubes as an introducer and using the curve-tipped suction catheter as a guidance during the nasotracheal intubation are also newly introduced techniques for safe nasotracheal intubation [3,4,9].
Since various methods exist, a safer procedure can be performed by using an appropriate method according to the operator's preference, clinical conditions, and skill level.
In conclusion, it seems that several redirections of the nasal tube may cause significant trauma of structures in the nasal cavity and could be asymptomatic during the immediate period. Checking the soundness of nasal structures is recommended when multiple efforts were made even if there were no signs of bleeding. And anesthesiologists should place the tube in the lower pathway of the nostril, and some techniques for safe insertion such as prewarming the tube could also be considered.


