서 론
림프관종(lymphangioma)은 소아에서 호발하는 양성 종양이다. 주로 두부, 경부, 액와부에 잘 생기며, 편평한 내피세포, 림프구 군집 및 결합조직 등이 낭성 구조물을 형성한다[1]. 성인 장중첩증(intussusception)은 전체 장중첩증 중에서 5%–10%의 비중을 차지하며, 복부 팽만감, 복통, 구역, 구토, 혈변, 빈혈 등 다양한 비특이적 증상들을 나타낸다[2,3]. 성인 장중첩증의 원인으로 지방종, 선종, 암종 등의 종양 및 수술 후 합병증 등이 보고되고 있으나, 림프관종에 의한 성인 장중첩증은 매우 드물다[4-6]. 저자는 맹장 림프관종에 의해 발생한 성인 장중첩증 1예를 경험하였기에 문헌고찰과 함께 보고하는 바이다.
증 례
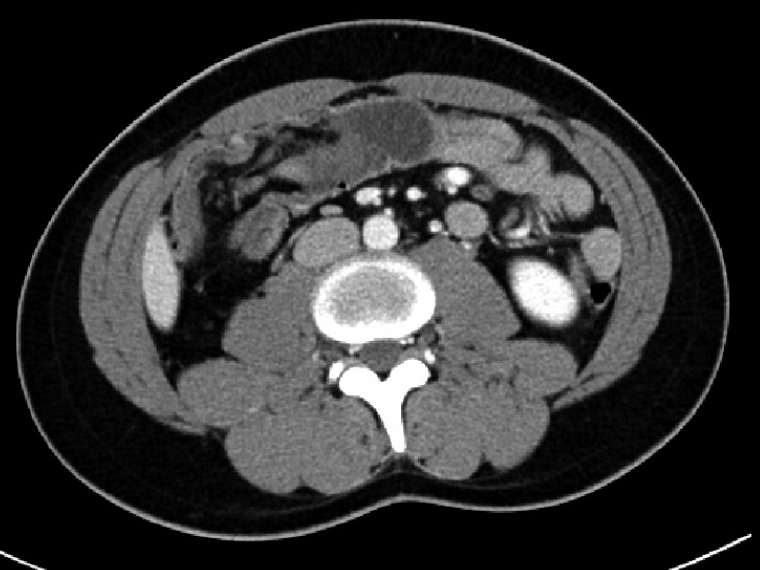
21세 남자 환자가 내원 1일 전 급성 복통을 주소로 내원하였다. 본 환자는 2014년 장중첩증으로 치료(laparoscopic exploration)받은 과거력이 있는 환자로 증세가 당시와 유사하다고 호소하였다. 내원 당시 혈압 110/90 mm Hg, 심박 수 73회/분, 호흡수 20회/분, 체온 37.2도로 측정되었고, 신체검사상 우측 복부에 지속적이고 찌르는 듯한 압통을 호소하였다. 혈액검사상 백혈구 수가 13,570/μL로 증가되어 있었고, 소변검사상 특이소견은 없었다. 흉부 X-ray상 특이소견 없었고, 응급으로 시행한 복부 전산화 단층촬영(abdominopelvic computed tomography)상 우측 복부 장중첩증 및 경도의 비장비대증(splenomegaly)이 관찰되어(Fig. 1), 정확한 진단 및 치료를 위해서 복강경 회맹장 절제술(laparoscopic ileocecectomy)을 시행하였다.
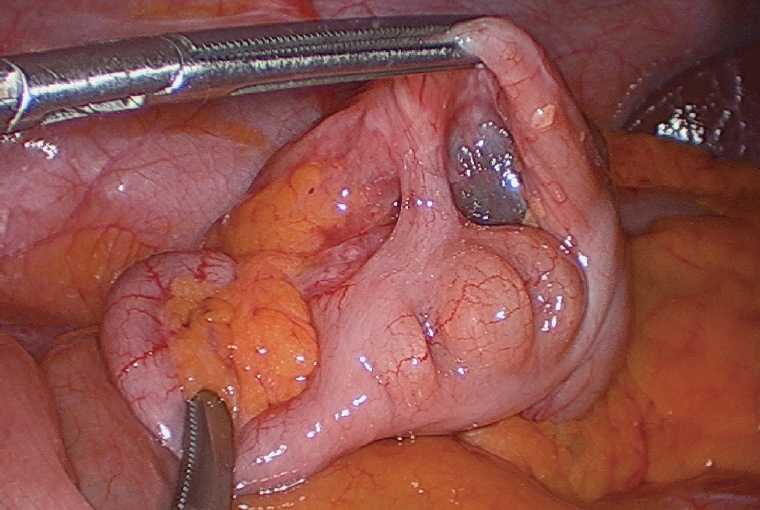
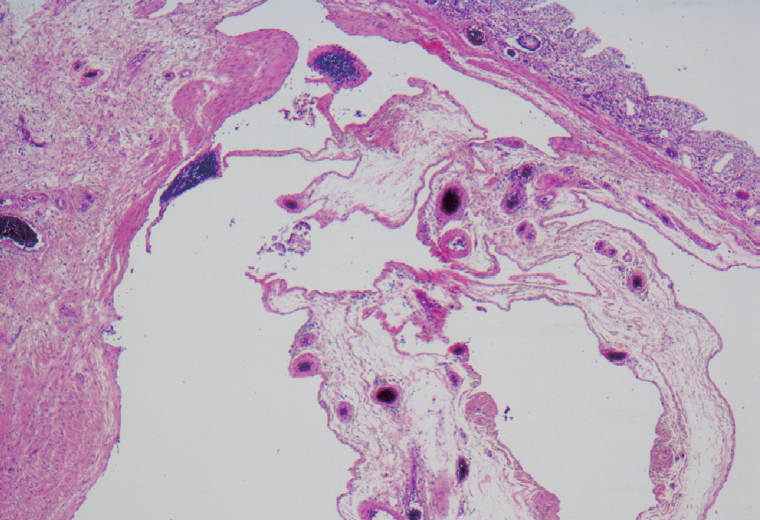
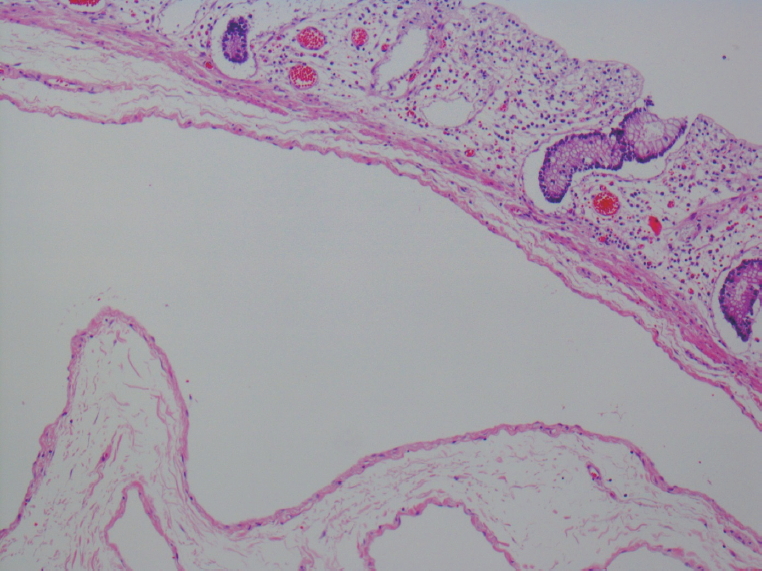
복강경검사상 회맹장 부위에 장중첩증이 발견되었고, 맹장 부위에 5×5 cm 크기의 둥글고 부드러운 경계를 가진 점막하 종양(submucosal lesion)이 관찰되었다(Fig. 2). 복강경 회맹장 절제술을 통해 병변을 제거하고 조직 생검을 실시하였다. 조직병리학적 검사상, 점막은 특이소견이 관찰되지 않았고, 점막하 부위에 맑은 림프액을 가진 다양한 크기의 낭성 병변과 산재된 림프구 군집들이 국소적으로 관찰되었다(Fig. 3). 확장된 낭성 병변의 벽은 편평한 양성의 내피세포들로 둘러싸여져 있었다(Fig. 4). 면역조직화학검사상 D2-40에서 양성 소견을 보였고, CD31, CK 등에서는 음성 소견을 보였다(Fig. 5). 이러한 소견들을 종합하며 본 증례는 맹장 림프관종에 의해 발생한 장중첩증으로 최종 진단되었다.
이 보고서의 출판을 위해 환자로부터 서면동의(informed consent)를얻었다.
고 찰
성인 장중첩증의 경우 전체 장중첩증 중에서 5%–16%를 차지하고, 복통, 구역, 구토, 혈변, 흑색변, 빈혈, 설사 등 급성 및 만성의 비특이적 증상들을 보인다. 임상양상이 급성 맹장염이나 장폐색증과 유사하므로 감별에 유의해야 한다[7]. 대장 장중첩증(colonic intussusceptions)의 가장 흔한 양성 원인으로 지방종(lipoma), 선종(adenoma) 등이 있으며, 본 증례처럼 림프관종에 의해 발생한 대장 장중첩증은 매우 드물다[4,5]. 장중첩증의 진단을 위해 복부 초음파(abdominal sonography), 바륨 관장(barium enema), 복부 전산화 단층촬영, 복강경검사(laparoscopic exploration) 등이 이용된다. 초음파검사상 transverse view에서 target sign, longitudinal view에서 pseudo-kidney sign이특징적이고, 바륨관장검사에서는 cup-shaped filling defects와 spiral or coil-spring appearance가 특징적이다. 복부 전산화 단층촬영이 특히 유용한데, layered effect를 동반한 inhomogeneous, target or sausage-shaped soft tissue mass 소견이 특징적이다[7,8].
림프관종은 일종의 혈관성 기형(vascular malformation)으로서 두부, 경부, 액와부등에서잘생긴다. 복강내에서발생할경우 mesentery에서 가장 호발하고, 그 외에 omentum, retroperitoneum, mesocolon, pancreas, spleen, adrenal gland 등에서도 발견된다[9]. 형태학적으로 모세혈관성(capillary), 해면성(cavernous), 낭성(cystic) 병변으로 분류하기도 하며, 5세 이하 소아에서 호발한다. 발생기전은 잘 알려져 있지 않으나, blind-ended lymphatic sac 증식 및 확장 같은 선천적 결함, 복강 내 손상, lymphatic degeneration 혹은 obstruction 등이 일부 관여한다고 알려져 있다[10]. 대장에서 발생한 낭성 림프관종은 매우 드문 편으로, 최근까지 79개 정도의 증례가 보고되었다[11]. 무증상인 경우가 많기 때문에 대장내시경(colonoscopy)이나 바륨 관장검사를 하면서 우연히 발견되는 경우가 많고, 주로 횡행 결장(transverse colon) 및 상행 결장(ascending colon)에서 발견된다. 증상으로 간헐적 복통, 복부 팽만감, 설사, 혈변 및 단백소실 장병증(protein-losing enteropathy) 등이 있다[12]. 대장내시경검사상 부드러운 표면을 가진 반투명의 압축성 용종성 병변으로 관찰되는 경우가 많다. 조직병리학적 검사상 점막은 온전한 편이며, 점막하 부위에 양성의 내피세포들로 둘러싸인 확장된 림프관 채널들이 관찰되고, 기질 내에 산재된 림프구 군집들이 국소적으로 발견된다. 감별 진단으로는 lipoma, leiomyoma, cavernous hemangioma, carcinoid tumor, mucocele 등이 있다[13]. 치료는 병변의 크기가 2 cm 이내로 작고 합병증이 동반되지 않은 경우 치료적 내시경(therapeutic colonoscopy)이 권장된다. 크기가 2 cm 이상으로 크거나 장중첩증, 혈변, 단백소실장병증 등의 합병증이 동반될 경우 치료적 내시경은 장천공 등의 위험이 있으므로 segmental resection, wedge resection 같은 외과적 절제술을 시행한다[4,5]. 본 증례는 림프관종의 크기가 5×5 cm로 큰 편이었고, 장중첩증, 복통 등의 합병증이 동반되었기 때문에 복강경 회맹장 절제술을 시행하였다.