서 론
배꼽창자간막관(omphalomesenteric duct)은 태생기 초기에 난황낭(yolk sac)과 태아의 원시 중간창자(primitive midgut)를 연결하며, 대부분 태생기 6주에 폐쇄되며, 정상적인 퇴축이 정지되는 단계에 따라 여러 가지 이상이 동반된다[1]. 영유아의 약 1%–4%는 폐쇄되지 않고 남아있어 이들 중 소수에서 여러 가지 합병증을 유발한다[2]. 합병증은 대부분 2세 이전에 나타나며 나이가 많아질수록 감소하는 것으로 알려져 있다[1]. 아기의 제대에서 혈청, 담즙, 태변성 분비물이 보이는 경우 배꼽창자간막관이 남아 샛길을 형성하고 있는 것을 의심할 수 있다[3]. 이러한 개방성 배꼽창자간막관(patent omphalomesenteric duct)은 보고된 바가 드문 질환이다. 저자들은 출생 후 제대에서 태변 배출이 확인된 신생아에게서 개방성 배꼽창자간막관으로 진단하고 수술로 완치한 1예를 보고하는 바이다.
증 례
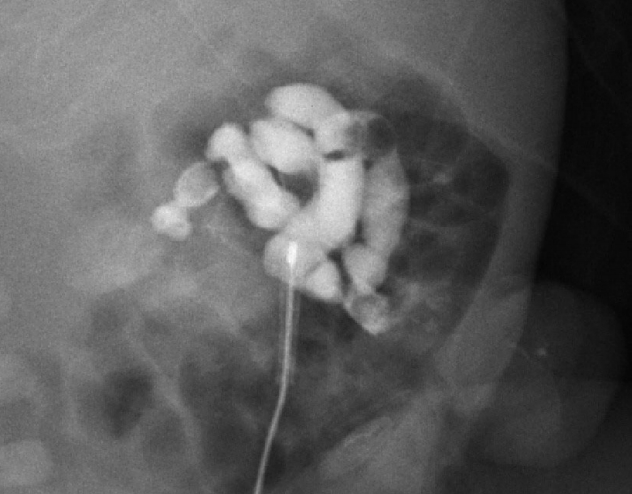
환아는 순천향대학교 천안병원에서 33세 산모의 첫째 남아로 재태 34주 6일에 출생체중 2,250 g으로 산모의 조기양막파수, 조기진통이 있어 응급 자연분만으로 출생하였다. 아프가점수(Apgar score)는 1분에 6점, 5분에 8점이었다. 출생 당시 전신에 태변 착색이 있었고 2회의 경부제대(nuchal cord)가 있었다. 신체검진에서 복벽의 이상과 항문의 이상은 없었다. 결찰된 제대의 근위부에는 태변 배출이 보이는 0.3 cm 크기의 열린 장관모양의 샛길(fistula)이 확인되었다(Fig. 1). 이 구조물은 산전 초음파검사에서는 발견되지 않았다. 다른 신체검진에서 특이점은 없었다. 복부 방사선사진에서 대장에 공기음영이 없이 소장의 공기음영은 관찰되었으나 소장의 확장소견은 의심되지 않았고 복강 내 종괴를 의심할 소견은 없었다. 복부초음파검사에서 소장의 일부가 제대로 탈장되어 있고 약 0.3 cm 굵기의 샛길로 연결되어 있었다. 장관조영검사를 시행하였고 조영제를 제대점막으로 돌출된 샛길을 통해 주입하였고 조영제가 소장으로 통과되는 것을 확인하였다(Fig. 2). 생후 2일에 시행한 심장초음파에서는 동맥관 개존과 난원공 개존이 관찰되었으나 연령을 고려하여 정상적인 구조로 여겨졌다. 특이 심기형은 없었고 가슴사진과 심전도검사에서 특이소견이 없었다.
출생 2일째 제대 위쪽을 횡절개하여 개복술을 시행하였다. 개복 후 돌막창자판막(ileocecal valve) 상방 20 cm 위치에서 제대를 향해 탈장되어 제대표면과 샛길이 형성된 배꼽창자간막관을 확인하였다(Fig. 3). 제대에 절개를 가하여 탈장된 배꼽창자간막관을 복강쪽으로 꺼내고 배꼽창자간막관의 근위부에서 회장의 일부를 포함한 구획절제술(segmental resection) 후 단단문합술(end-to-end anastomosis)을 시행하였다. 복강 내 다른 이상이 없음을 확인하고 배꼽축소술(umbilicoplasty)을 시행 후 배액관을 거치하고 복강 내 수술을 완료하였다. 환아는 수술 후 신생아중환자실에서 5일간 금식 후 수유를 시작하였다. 이후 시행한 선천성 대사이상선별검사에서 특이점이 없었고 염색체검사에서 46,XY 정상이었으며 난청검사, 망막검진에서도 특이점이 없었다. 환아는 출생 21일째 다른 합병증 없이 퇴원하였다.
고 찰
태내에서 태아는 태반이 형성될 때까지 난황낭으로부터 영양을 공급받는다. 재태 2–4주 사이에 원시 난황낭(primitive yolk sac)은 원시장(primitive gut)과 고유난황낭(yolk sac proper)으로 나뉘어져 서로 교통하여 배꼽창자간막관이 발생한다[2]. 그 이후 태반에서 영양이 공급되면서 배꼽창자간막관은 임신 6–8주 사이에 제대 부위로부터 폐쇄가 시작되어 소장 쪽으로 진행하여 막히게 된다[4]. 이러한 퇴축과정의 이상으로 여러 가지 배꼽창자간막관 폐쇄기형이 인구의 약 2%에서 나타난다[2]. 1959년 Soderlund [5]는 이러한 폐쇄과정의 이상에 따라 메켈게실, 배꼽창자간막관낭종, 게실간막띠, 제대용종, 제대동(omphalomesenteric cyst), 완전개방성 배꼽창자간막관(patent omphalomesenteric duct)으로 6가지 형태의 배꼽창자간막관 폐쇄기형을 분류하였다[5]. 이 중 메켈게실이 65%–80%로 가장 흔하며, 게실간막띠는 약 11%를 보이고, 완전개방성 배꼽창자간막관이 가장 드문 것으로 알려져 있다[5]. 대부분 무증상이나 증상이 나타날 경우 복통, 직장출혈, 제대배액(umbilical drainage), 배꼽탈장 등의 증상이 연령에 따라 다르게 나타난다. 대부분 증상은 4세 이전에 나타나며 1개월 미만의 신생아의 85%, 1–2세 유아의 77%에서 증상이 나타난다[6]. 동반 기형으로는 장관폐쇄, 심장기형, 구순구개열이 있을 수 있으며, 13번 삼염색체증과 다운증후군에서도 배꼽창자간막관 폐쇄기형이 동반될 수 있다[7].
완전개방성 배꼽창자간막관의 경우 개방관을 통한 회장의 팽출 또는 외반이 일어날 수 있는 위험성이 높다. Kling [8]에 의하면 개방성 배꼽창자간막관은 장폐쇄와 혈관장애가 급속히 동시에 일어날 수 있는 사망률이 높은 질환으로 탈장의 여부를 막론하고 발견 즉시 수술하는 것은 권하였다.
산전 초음파에서 단순 배꼽탈장은 쉽게 발견되며 배꼽창자간막관 낭종 역시 드물지 않게 확인할 수 있다. 하지만 개방성 배꼽창자간막관의 산전 초음파 진단은 어렵고 그 경우가 매우 드물다[9]. 대부분 출생 후 초음파검사 또는 장관조영검사로 진단하며 진단 즉시 수술적 절제가 추천된다[6,8].
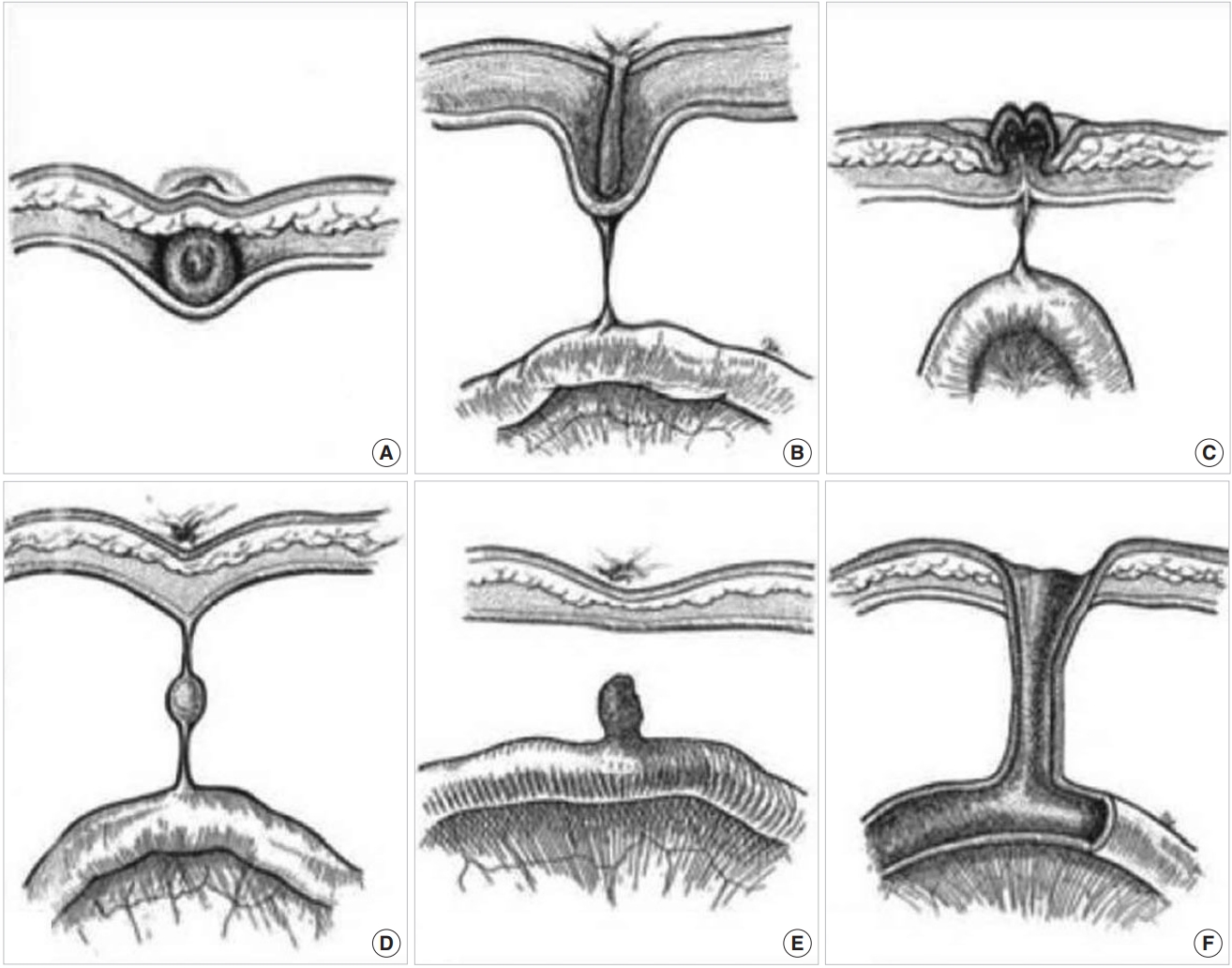
본 증례의 환아도 남아로 산전 초음파검사에서는 확인되지 않았고 출생 직후 제대의 샛길을 통하여 태변배출이 있어 개방성 배꼽창자간막관을 의심하여 초음파검사와 샛길을 통한 장관조영검사로 확인 후 즉시 수술적 절제를 시행하여 확진 및 치료하였다. Fig. 4에서는 여러 가지 배꼽창자간막관 잔유물의 형태를 보여주고 있으며[10], 본 증례에서 수술을 통하여 Fig. 4F 형태의 개방성 배꼽창자간막관을 확인할 수 있었다.
출생 시 제대에 대한 세심한 관찰이 필요하며, 만약 배꼽탈장이 있으면서 제대주위 염증이 반복되거나 제대를 통한 담즙성 분비물 또는 간헐적인 출혈이 보이는 경우 배꼽창자간막관 폐쇄기형을 고려해야 한다. 특히 샛길을 통한 태변배출이 확인된다면 개방성 배꼽창자간막관 샛길을 고려하여 합병증 예방을 위해 즉시 수술적 절제를 시행하는 것이 중요하다.