SMS 2012 June;18(1):52-55.
Published online 2012 July 17 |
| Copyright ⓒ 2010 Soonchunhyang Medical Science
|
| A Case of Delayed Fatal Hemobilia after Radiofrequency Ablation of Hepatocellular Carcinoma |
| Seung Kyu Chung, Baek Gyu Jun, Sae Hwan Lee, Suck-Ho Lee, Il-Kwun Chung, Hong Soo Kim, Sang-Heum Park, Sun-Joo Kim |
| Division of Gastroenterology/Hepatology, Department of Internal Medicine, Soonchunhyang University College of Medicine, Cheonan, Korea |
| Corresponding Author: Hong Soo Kim , Tel: +82-41-570-3676 , Fax: +82-41-574-5762 , Email: khskhs@sch.ac.kr
|

|
ABSTRACT
|

|
|
| Radiofrequency ablation (RFA) has been accepted as a safe and effective treatment for unresectable hepatic tumors because of the advantages of a minimally invasive procedure and the local treatment effect. Although RFA can be performed safely in most patients, early and late complications related to mechanical or thermal damage may be observed at follow-up examination. Hemobilia is a very rare complication of RFA and most hemobilia is an immediate complication. However, delayed hemobilia is an even more rare complication after RFA and is known to be a fatal complication. We present a case of delayed fatal hemobilia after RFA for hepatocellular carcinoma. |
|
Keywords: Radiofrequency ablation; Hemobilia; Hepatocellular carcinoma |
|
|
|
INTRODUCTION
|
|
|
| Radiofrequency ablation (RFA) is performed for unresectable hepatocellular carcinoma (HCC) and metastatic liver tumor more widely than other local treatment because it results in large coagulated necrosis of the tumor, requires fewer treatment session, and achieves higher survival rates
[1]
. Even though radiofrequency ablation is known to be a safe procedure, it is known that about 2.2% of patients experienced a major complication and about 0.3% of patients died according to a multi-center study
[2]
. Hemobilia is a very rare complication of RFA, occurs about 0.25% after RFA, mostly shows within 4 days after the procedure and is improved by conservative treatment
[3]
. However, delayed hemobilia is an even more rare complication after RFA and is known to be a fatal complication although it has been reported in only one case
[4]
. We experienced a case of delayed fatal hemobilia after RFA for HCC. |
|
|
CASE REPORT
|
|
|
A 58 year-old female patient was admitted with a complaint of chest pain. She was diagnosed with 2-vessel disease and underwent a percutaneous coronary intervention. Laboratory test results were as follows: white blood cell, 4,500/mm3; hemoglobin, 11.1 g/dL; platelet, 82×103/μL; aspartate aminotransferase (AST), 20 IU/L; alanine transaminase (ALT), 19 IU/L; albumin, 3.7 g/dL; total bilirubin, 0.8 mg/dL; prothrombin time (PT) international normalized ratio (INR), 1.01; α-fetoprotein, 64.3 ng/mL; HBsAg/ anti-HBs,+/-; HbeAg/Anti-HBe, -/+; and HBV DNA, negative. Abdomen ultrasonography was performed, which revealed a 2.0 cm hepatic mass located in segment V. The patient was diagnosed with HCC through liver computed tomography (CT) during both arterial portography and hepatic arteriography
(Fig.1)
. RFA was selected due to the patient’s refusal of hepatic resection or liver transplantation. She had stopped taking an antiplatelet agent 5 days prior the RFA, in order to reduce the risk of bleeding. Two days after RFA, abdomen CT showed no complications, including bile duct injury
(Fig.2)
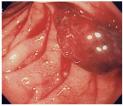
. Five days after RFA, she was discharged without any complications and restarted the antiplatelet agent. Twenty-three days after RFA, she was admitted again with complaints of nausea, vomiting and pain in the right upper quadrant of the abdomen. Her vital signs were as follows: blood pres-sure, 110/80 mmHg; pulse rate, 76 beats/min; respiration rate, 17 breaths/min; and body temperature, 36.5°C. Melena or hematemesis was not observed from a systematic view, while the tenderness in the right upper quadrant and jaundice was noted by physical examination. Laboratory test results were as follows: white blood cell, 22,700/mm3; hemoglobin, 8.4 g/dL; platelet, 96×103/μL; AST, 161 IU/L; ALT, 105 IU/L; albumin, 2.9 g/dL; total bilirubin, 2.6 mg/dL; alkaline phosphatase, 362 IU/L; γ-glutamyl transpeptidase, 413 IU/L; and PT INR, 1.33. Colonoscopy, abdominal ultrasonography, and liver CT were performed to evaluate complications from RFA, such as hemoperitoneum, intrahepatic abscess, or gastrointestinal perforation. However, no complications were found except for ischemic colitis due to colonscopy. Therefore, conservative treatment was instituted and the patient stopped taking the antiplatelet agent. Thirty-five days after RFA, massive hematochezia occurred when blood pressure dropped to 90/60 mm Hg, with an increased pulse rate of 98 beats/min. On gastroduodenoscopic examination, the esophagus, stomach and duodenal bulbus showed no active bleeding, but a bleeding point was found at the papilla of Vater
(Fig.3)
. Angiography was performed to confirm hemobilia; however, there was no active bleeding point in angiography. Hemobilia was suspected because bile duct dilatation and aspiration of hematomas were observed during percutaneous transhepatic biliary drainage
(Fig.4)
.
The patient received conservative treatment and the massive hematochezia improved. However, the patient then developed respiratory, kidney and liver failures. Five days after the onset of hemobilia and 40 days after RFA, the patient died. |
|
|
DISCUSSION
|
|
|
RFA is an efficient local treatment for unresectable HCC [1,5]. It has been considered as a treatment option alternative to hepatic resection for cases where a tumor is less than 3 cm
[6]
. However, complications may occur after the procedure. Livraghi et al.
[2]
have reported that, after RFA, the incidence of major complications is 2.2% and the mortality rate is 0.3%. The most frequent complication is hemoperitoneum. In addition intrahepatic abscesses and needle-track seeding of HCC can also occur after RFA. The most common causes of death are intraperitoneal infections by intestinal perforation and multiorgan failures. Other causes include hepatoma rupture and bile duct injuries
[2]
. RFA produces thermal injuries to peripheral tissue and the intrahepatic bile duct which can cause bile duct complications, such as biloma, bile duct stenosis and hemobilia. Thermal injuries to the biliary tract should be considered when the HCC is located adjacent to the intrahepatic bile duct. Also, hepatic artery chemoembolization or percutaneous ethanol injection therapy should be considered at this time as well
[7]
. Intraductal chilled- saline perfusion has been reported to reduce the incidence of bile duct injuries
[8]
.
Hemobilia is a very rare complication after RFA. Rhim et al.
[3]
have reported that the incidence of hemobilia following RFA is 0.25% when RFA is performed. In most cases, melena and abdominal pain in the right upper quadrant are observed 1 to 4 days after RFA, and hemobilia after RFA improves with conservative treatment
[3]
. Moon et al.
[9]
have shown that hemobilia occurs within 1 day of RFA but improves with conservative treatment. There has only been 1 case of delayed hemobilia after RFA that turned out to be a fatal complication. In that case, the patient died 4 days after the onset of hemobilia and 39 days after RFA
[4]
.
Imaging studies, such as ultrasonography, should be performed when laboratory test results show decreased hemoglobin, increased bilirubin and biliary enzyme. Appearance of echogenic material in the gallbladder lumen is a useful early sign of hemobilia during ultrasonography
[10]
. Hemobilia can be diagnosed by endoscopy with hemorrhage in the ampulla of Vater. No treatment is necessary for asymptomatic patients, but endoscopic drainage may be required in patients with significant jaundice. Transcatheter arterial embolization can be performed to stop bleeding from pseudoaneurysms or fistulas
[8]
. In our case, delayed hemobilia after RFA appeared to be the fatal result in a patient with 2-vessel disease of the coronary artery who received a percutaneous coronary intervention and was taking an antiplatelet agent with high risk of he-morrhage. She was readmitted 23 days after RFA with complaints of nausea, vomiting and abdominal pain in the right upper quadrant, and was further evaluated for a biliary tract injury because cholestasis was suspected based on the laboratory test results. However, she received only conservative treatment because there was no evidence of biliary tract injury on the CT at that time. This led to the delayed diagnosis of hemobilia. Additionally, bleeding was not stopped with transcatheter embolization in the early stage because pseudoaneurysms or fistulas were not found. Therefore, multiorgan failure was caused by a massive hemorrhage.
Since RFA continues to be performed in unresectable HCC cases and antiplatelet agents, such as aspirin, are increasingly being taken, the incidence of delayed hemobilia may increase. When a delayed gastrointestinal tract bleeding occurs after RFA, hemobilia should be differentiated so that an early treatment, such as transcatheter embolization and endoscopic drainage, may be performed to treat hemobilia. In our case, the patient restarts taking the anti-platelet agent 5 days of RFA due to high risk of stent restenosis. In particular, when gastrointestinal tract bleeding does not appear but is suspected from laboratory test results or clinical symptoms/signs in patients who are taking antiplatelet agents or biliary tract injuries, clinicians should carefully evaluate complications of RFA, including hemobilia.
We experienced the case of a patient with delayed fatal hemobilia that occurred after RFA for HCC and reported it with a literature review to help clinicians manage patients who undergo RFA. In conclusion, it is suggested that clinicians should carefully observe delayed hemobilia after RFA in HCC patients who are on taking anti-platelet agents or who are suspected of having suspected biliary tract injuries. |
|
|
|
FIGURES
|
|
|

|
Fig.1
(A) Initial abdominal computed tomography (CT) at the arterial phase obtained before radiofrequency ablation shows a 2 cm hyper-attenuating mass in segment 5. (B) Abdominal CT scan shows contrast wash out in the mass at the delayed phase. |

|

|
Fig.2
Follow-up abdominal computed tomography scan obtained 2 days after radiofrequency ablation shows a 5 cm hypo-attenuating lesion in segment 5 due to radiofrequency ablation and with no evidence of bile duct injury. |
|
|
|
Fig.3
Esophagogastroduodenoscopy shows a large hematoma oozing from the ampulla of Vater. |
|
|

|
Fig.4
Percutaneous transhepatic biliary drainage of bloody material was performed through the left lateral segmental duct. The common bile duct is dilated. |
|
|
|
| |
|
|
REFERENCE
|
|
|
|
1.
|
Yan K, Chen MH, Yang W, Wang YB, Gao W, Hao CY, et al. Radiofrequency ablation of hepatocellular carcinoma: long-term outcome and prognostic factors. Eur J Radiol 2008;67:336-47. |
|
2.
|
Livraghi T, Solbiati L, Meloni MF, Gazelle GS, Halpern EF, Goldberg SN. Treatment of focal liver tumors with percutaneous radio-frequency ablation: complications encountered in a multicenter study. Radiology 2003; 226:441-51. |
|
3.
|
Rhim H, Lim HK, Kim YS, Choi D, Lee KT. Hemobilia after radiofrequency ablation of hepatocellular carcinoma. Abdom Imaging 2007;32: 719-24. |
|
4.
|
Enne M, Pacheco-Moreira LF, Cerqueira A, Balbi E, Pereira JL, Martinho JM. Fatal hemobilia after radiofrequency thermal ablation for hepatocellular carcinoma. Surgery 2004;135:460-1. |
|
5.
|
Gazelle GS, Goldberg SN, Solbiati L, Livraghi T. Tumor ablation with radio-frequency energy. Radiology 2000;217:633-46. |
|
6.
|
Lau WY, Lai EC. The current role of radiofrequency ablation in the management of hepatocellular carcinoma: a systematic review. Ann Surg 2009; 249:20-5. |
|
7.
|
Rhim H, Yoon KH, Lee JM, Cho Y, Cho JS, Kim SH, et al. Major complications after radio-frequency thermal ablation of hepatic tumors: spectrum of imaging findings. Radiographics 2003;23:123-34. |
|
8.
|
Ohnishi T, Yasuda I, Nishigaki Y, Hayashi H, Otsuji K, Mukai T, et al. Intraductal chilled saline perfusion to prevent bile duct injury during percutaneous radiofrequency ablation for hepatocellular carcinoma. J Gastroenterol Hepatol 2008;23(8 Pt 2):e410-5. |
|
9.
|
Moon JS, Kim HJ, Kim SJ, Moon HJ, Lee HW, Choi CH, et al. Hemobilia after radiofrequency ablation of hepatocellular carcinoma. Korean J Hepatol 2007;13(3 Suppl):196A. |
|
10.
|
Obi S, Shiratori Y, Shiina S, Hamamura K, Kato N, Imamura M, et al. Early detection of haemobilia associated with percutaneous ethanol injection for hepatocellular carcinoma. Eur J Gastroenterol Hepatol 2000;12:285-90. |
|
|
|











