소아 뇌동정맥기형 치료 후 새로 발생한 뇌동정맥기형
ABSTRACT
The cerebral arteriovenous malformation (AVM) recognized as a congenital lesion traditionally. AVM is an abnormal connection between cerebral artery and vein without capillary and neural structure. Nidus of AVM was located between arteriovenous direct connections. This case report presents newly developed de novo AVM after curative treatment of the initial AVM lesion. The 8-year-old boy was admitted with a small intracranial hemorrhage on medulla oblongata and intraventricular hemorrhage. Nidus of AVM was found on medulla oblongata by trans-femoral cerebral angiography (TFCA). Nidus’s embolization using Oynx (Medtronic, Minneapolis, MN, USA) was performed and complete occlusion was maintained for 4 years. Newly developed AVM was found on a 4-year follow-up TFCA. The de novo AVM is located opposite hemisphere from the initial AVM. New AVM was treated by radiosurgery, and the treatment result is being observed. The de novo AVM is a very rare condition. However, AVM may have a chance to develop in a new location and physicians may have attention to de novo AVM.
Key words: Intracranial arteriovenous malformation; Embolization; Angiography
서 론
뇌동정맥기형은 비정상적인 뇌동맥과 뇌동정맥 간의 연결이 이루어져 발생하는 질환으로, 뇌조직으로 가는 모세혈관조직을 거치지 않고 뇌동맥이 뇌정맥으로 단락(shunting)되는 구조를 가진다[ 1]. 뇌동정맥 기형은 발생하는 위치 또는 크기, 모양, 정맥의 배출위치(drainage vein)에 따라 다양한 형태와 임상증상, 예후를 갖게 된다. 뇌동정맥기형은 병태생리상 선천적인 기형으로 알려져 있다[ 2]. 이 증례에서는 소아 환자에서 최초 뇌간에 발생한 뇌동정맥을 치료한 이후 소뇌에 이전에 없던 새로운 뇌동정맥기형이 발견되어 보고하고자 한다.
증 례
8세 남자 환자가 내원 1일 전부터 발생한 10회 이상의 구토, 두통, 전신 쇠약감을 주소로 응급실로 내원하였다. 응급실에서 최초 시행한 두부 컴퓨터단층촬영 영상에서는 뇌의 연수(medulla oblongata) 부위의 소량의 뇌 내 출혈 및 제4뇌실과 제3뇌실, 양측 측뇌실의 뇌실 내 출혈, 경한 수두증이 동반되어 있었다. 진단을 위해 시행한 대퇴동맥을 통한 뇌혈관조영술에서는 좌측 척추동맥의 경추 1번, 2번 사이 분절(V3 segment, 두개 외 분절)에서 기시하는 공급동맥(feeding artery)을 통해 뇌연수 부위(10 mm×8 mm)에 뇌동정맥기형의 핵(nidus)이 관찰되었으며, 동정맥기형에 의해 유발된 동맥류(6.7 mm×5.3 mm)가 뇌동정맥기형의 핵(nidus) 부위에 근접하여 관찰되었다(Spetzler-Martin 2등급). Onyx (Medtronic, Minneapolis, MN, USA)를 이용한 뇌동정맥기형의 색전술을 시행하여 공급동맥 및 핵, 배출정맥의 혈류차단을 확인하였다( Fig. 1A, B). 환자는 외과적 시술 및 포괄적 재활치료를 시행하고 45일 만에 퇴원하였으며, 퇴원 후 17개월 뒤 시행한 대퇴동맥을 통한 뇌혈관조영술에서도 재발은 관찰되지 않았다. 4년 뒤 어지러움 증상이 새로 발생되어 시행한 두부 자기공명영상의 T2 영상에서 우측 소뇌의 피질하(subcortical) 부분에 높은 신호강도 병변이 1 cm 크기로 관찰되었으며, 주변에 공급동맥으로 보이는 비정상 혈관의 신호공백(signal void)이 관찰되었다. 진단을 위해 시행한 대퇴동맥을 통한 뇌혈관조영술에서 우측 후하소뇌동맥의 말단에서 기시하는 공급동맥이 관찰되었으며, 8 mm×4 mm 크기의 뇌동정맥기형의 핵과 뇌동정맥기형에 의해 유발된 9.5 mm×6.5 mm 크기의 미파열성 동맥류가 근접하여 관찰되었다. 배출정맥은 단일정맥으로 우측 소뇌피질 쪽으로 배출되었다(Spetzler-Martin 1등급) ( Fig. 2A, B). 새로 발견된 뇌동정맥기형은 방사선수술 시행 후 경과관찰 중이다. 이 증례연구의 출판을 위해 입원 당시 환자 보호자로부터 의학 정보의 연구자료 이용 동의를 얻었다.
고 찰
뇌동정맥기형은 현재까지 선천적인 병변으로 알려져 있다[ 2]. 뇌동정맥기형은 태아의 발생과정 중 매우 이른 시기에 형성(태아의 크기가 40에서 80 mm 크기일 때)되는 것으로 알려져 있다[ 3]. 이 기간에 뇌혈관이 성숙해지기 위해 여러 가지 발생학적 과정을 거치게 되며 이때 발생한 뇌동정맥기형이 신생아 시기에도 계속 존재하여, 일반적으로 임상증상을 나타내기 전까지는 무증상인 체로 존재한다고 알려져 왔다[ 4, 5]. 하지만 흔하지 않게 기존의 뇌동정맥기형과 관계없는 새로운 뇌동정맥기형이 발견되는 사례들이 증가하고 있다[ 6- 12]. 이렇게 선천적 뇌동정맥기형 발생설에 일치하지 않는 증례들이 보고되면서 뇌동정맥기형을 후천적인 발생으로 보는 의견이 제기되었다. 만약 뇌동정맥기형이 선천적이라고 하면, 태아시기나 신생아 시기에 종종 발견되는 다른 뇌혈관의 기형(예: 갈렌정맥의 기형)과는 다르게 뇌동정맥기형은 여러 가지 뇌영상 진단법이 발달하였음에도 불구하고 태아 시기나 신생아 시기에는 거의 발견이 되지 않는 다는 점이 모순이 된다는 것이다[ 13- 15]. 즉 뇌동정맥기형은 선천적으로 태아 시기에 이미 형성되는 것이 아니라 유전적인 영향력만을 가지고 있다가 환경적 요인이 맞물려 서로 상호작용을 하면서 후천적으로 발생한다는 것이다[ 2]. 뇌동정맥기형을 후천적으로 발생시킬 수 있는 환경적인 요인으로는 물리적 변화, 염증반응, 혈전생성반응, 호르몬 변화, 혈류역학적 자극 등이 거론되고 있다[ 16, 17]. 또 하나의 가능한 뇌동정맥기형의 후천적 생성기전은 뇌동정맥루(dural arteriovenous fistula)의 생성기전과 같은 기전이다[ 18]. 뇌동정맥루가 뇌정맥동(dural sinus)의 정맥혈전증(venous thrombosis) 이후에 발생하는 것처럼 뇌실질의 정맥혈전증이 뇌동정맥기형의 발생을 유발하는 방아쇠 역할을 한다는 이론이다[ 18]. 이렇듯 최초로 발견된 뇌동정맥기형을 치료한 이후에 새로운 신규 뇌동정맥기형이 발생하는 현상은 아직 명확한 기전이 밝혀지지는 않았다. 이번 증례 보고한 환자의 경우, 새로 발생한 뇌동정맥기형이 최초 발견된 뇌동정맥기형과는 전혀 다른 동맥에서 혈류공급을 받고 있으며, 배출정맥도 전혀 다르다. 또한 최초의 뇌동정맥기형의 진단검사와 시술 후 완치 여부 판정을 위해 시행한 뇌혈관조영술에서는 새로운 뇌동정맥기형이 관찰되지 않았고, 새롭게 어지러움 증상이 생겨, 이에 대한 검사 중 새로운 신규 뇌동정맥기형이 발견되었다. 이는 환자에게 치료 중 발생한 여러 가지 뇌의 환경적 변화 요인에 의해 새로운 신규 뇌동정맥기형이 후천적으로 발생하였을 가능성도 고려해볼 수 있다. 흔하지는 않지만 뇌동정맥기형이 발견된 환자의 경우에는 차후 새로운 뇌동정맥기형의 발생 가능성에 대해 충분히 고려하며 치료 및 경과관찰을 해야 한다.
Fig. 1.
(A) Abnormal blood flow was observed on a left vertebral artery and arteriovenous malformation was well defined on the medulla oblongata. (B) Nidus was occluded completely after Onyx embolization. 
Fig. 2.
(A) The right cerebella hemisphere was normal in the 1-year follow-up angiography. (B) New arteriovenous malformation of the right cerebella hemisphere was defined in the 4-year follow-up angiography. 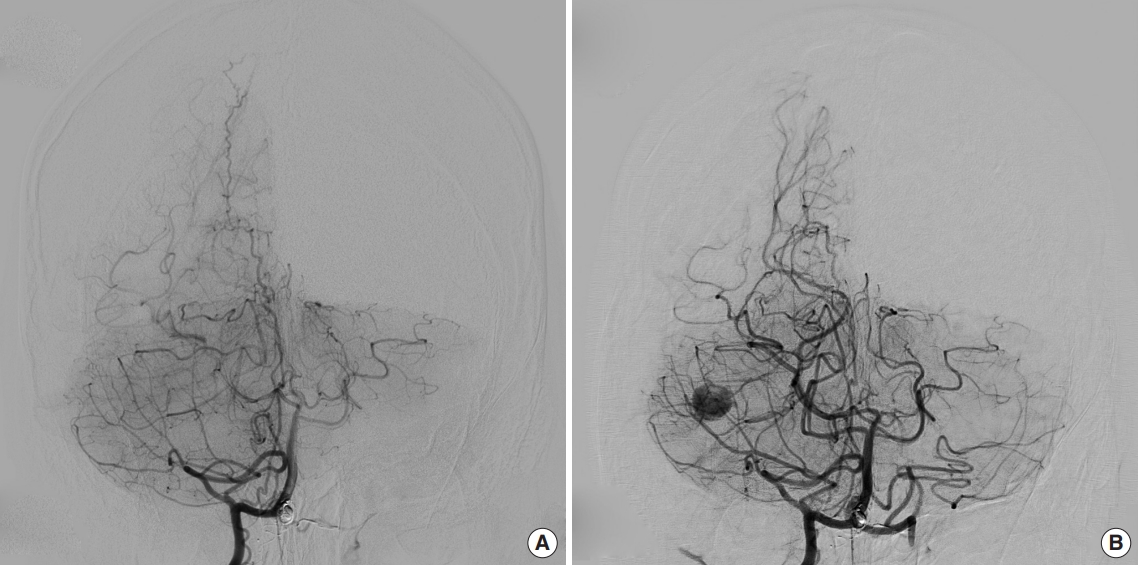
REFERENCES
1. Farhat HI. Cerebral arteriovenous malformations. Dis Mon 2011;57: 625-37.   2. Morales-Valero SF, Bortolotti C, Sturiale C, Lanzino G. Are parenchymal AVMs congenital lesions? Neurosurg Focus 2014;37: E2. 3. Mullan S, Mojtahedi S, Johnson DL, Macdonald RL. Embryological basis of some aspects of cerebral vascular fistulas and malformations. J Neurosurg 1996;85: 1-8. 4. Al-Shahi R, Bhattacharya JJ, Currie DG, Papanastassiou V, Ritchie V, Roberts RC, et al. Prospective, population-based detection of intracranial vascular malformations in adults: the Scottish Intracranial Vascular Malformation Study (SIVMS). Stroke 2003;34: 1163-9.
5. Stapf C, Mast H, Sciacca RR, Berenstein A, Nelson PK, Gobin YP, et al. The New York Islands AVM Study: design, study progress, and initial results. Stroke 2003;34: e29-33. 6. Akimoto H, Komatsu K, Kubota Y. Symptomatic de novo arteriovenous malformation appearing 17 years after the resection of two other arteriovenous malformations in childhood: case report. Neurosurgery 2003;52: 228-31. 7. Alvarez H, Perry V, Solle M, Castillo M. De novo cerebral arteriovenous malformation in a child with previous cavernous malformation and developmental venous anomaly. J Neurosurg Pediatr 2012;9: 327-30. 8. Bai Y, He C, Zhang H, Ling F. De novo multiple dural arteriovenous fistulas and arteriovenous malformation after embolization of cerebral arteriovenous fistula: case report. Childs Nerv Syst 2012;28: 1981-3. 9. O’Shaughnessy BA, DiPatri AJ Jr, Parkinson RJ, Batjer HH. Development of a de novo cerebral arteriovenous malformation in a child with sickle cell disease and moyamoya arteriopathy. Case report. J Neurosurg 2005;102(2 Suppl):238-43. 10. Rodríguez-Arias C, Martinez R, Rey G, Bravo G. Recurrence in a different location of a cerebral arteriovenous malformation in a child after radiosurgery. Childs Nerv Syst 2000;16: 363-5. 11. Schmit BP, Burrows PE, Kuban K, Goumnerova L, Scott RM. Acquired cerebral arteriovenous malformation in a child with moyamoya disease:case report. J Neurosurg 1996;84: 677-80. 12. Song JK, Niimi Y, Kupersmith MJ, Berenstein A. Postnatal growth and development of a cerebral arteriovenous malformation on serial magnetic resonance imaging in a child with hemangiomatosis: case report. J Neurosurg 2007;106(5 Suppl):384-7.
13. Auyeung KM, Laughlin S, Terbrugge KG. Prenatal diagnosis of unusual fetal pial arteriovenous malformation: a case report. Interv Neuroradiol 2003;9: 163-8. 14. DeCesare B, Omojola MF, Fogarty EF, Brown JC, Taylon C. Spontaneous thrombosis of congenital cerebral arteriovenous malformation complicated by subdural collection: in utero detection with disappearance in infancy. Br J Radiol 2006;79: e140-4. 15. Eguchi S, Aihara Y, Yamaguchi K, Okada Y. Limitations of fetal ultrasonography and magnetic resonance imaging in prenatal diagnosis of congenital cerebral arteriovenous malformations with hemorrhagic onset. J Neurosurg Pediatr 2012;10: 154-8. 16. Bulsara KR, Alexander MJ, Villavicencio AT, Graffagnino C. De novo cerebral arteriovenous malformation: case report. Neurosurgery 2002;50: 1137-40. 18. Aboian MS, Daniels DJ, Rammos SK, Pozzati E, Lanzino G. The putative role of the venous system in the genesis of vascular malformations. Neurosurg Focus 2009;27: E9. 
|
|











